Download
1 / 22
220 likes | 378 Views
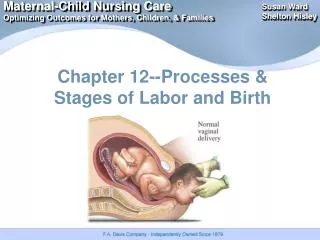
Labor and the birth. -Term for twins is usually considered to be 37 weeks rather than 40 - and approximately 50% of twins are born pre-term, that is before 37 weeks' gestation. - the babies may be small for gestational age and prone to complications.

E N D
Labor and the birth • -Term for twins is usually considered to be 37 weeks rather than 40 • - and approximately 50% of twins are born pre-term, that is before 37 weeks' gestation. • - the babies may be small for gestational age and prone to complications.
- If preterm labour begins , given her drugs to inhibit uterine activity. • - Intravenous salbutamol and sulindac tablets are the drugs most commonly used. • - urinary tract infection should be treated with antibiotics. • - IOL at 38 weeks. If the first twin is in a cephalic presentation, a vaginal birth • but if the first twin is presenting not cephalic ,an electctive C.S is usually recommended
- monochorionic twin pregnancies are now being delivered by elective caesarean section due to the risks of TTTS and premature separation of placenta before the birth of the second twin
Management of labor • -Education during the antenatal period • -IOL usually occurs around 38 weeks' gestation • -The presence of complications such as PIH,IUGR or TTTS reasons for earlier induction. • -The majority of women expecting twins will go into labour spontaneously.
- dysfunctional labor in twin pregnancies, because of over distension of the uterus. • - continuous CTG of both fetuses ,with two external transducers • - once the membranes are ruptured, a scalp electrode on the presenting twin and an external transducer on the second. • -Uterine activity monitored.
-If CTG is not available, use of the Doptone or Sonicaid • -fetal heart checked by two staff member . • -no specific position during labor • -A birthing chair or a reclining chair
-Regional epidural block provides excellent analgesia, allows easier instrumental deliveries • -The use of Entonox analgesia may be helpful, either before the epidural is in situ or during the second stage.
-The mother should be encouraged to use relaxation technique. • -If fetal compromise occurs during labour , caesarean section. • -If uterine activity is poor, the use of intravenous oxytocin may be required once the membranes have been ruptured
- AROM provide good uterine activity but may need to be used in conjunction with intravenous oxytocin. • - The CTG will give a good indication of the pattern of uterine activity, • -fill partogram • -prepare nursery or neonatal ICU • -emotional condition must be considered.
Management of the birth • - the second stage of labour should be confirmed by a vaginal examination. • -The obstetrician, pediatric team and anesthetist should be present. • - the operating theatre should be ready to receive the mother • - Monitoring of both fetal hearts should continue until birth. Provided that the first twin is presenting by the vertex, the birth can be expected to proceed normally
- When the first twin is born, the time of birth and the sex are noted. • - This baby and cord must be labelled as ‘twin one’ immediately. • - bracelets should be checked with the mother or father before they are applied to the infant's wrist and ankle.
- The baby may be put to the breast as sucking stimulates uterine contractions. • -After the birth of the first twin, abdominal palpation is made to ascertain the lie, presentation and position of the second twin and to auscultate the fetal heart. • - If the lie is not longitudinal, an attempt may be made to correct it by external cephalic version
-If it is longitudinal, a vaginal examination is made to confirm the presentation. • - If the presenting part is not engaged it should be pushed into the pelvis by fundal pressure before the second sac of membranes is ruptured. • -The fetal heart must be auscultated again and a scalp electrode applied once the membranes are ruptured.
- If uterine activity does not recommence, intravenous oxytocin may be used to stimulate it. • -When the presenting part becomes visible, the mother should be encouraged to push with contractions to birth the second twin. • -The midwife should be aware that, owing to the reduced size of the placental site following the birth of the first twin, the second fetus may be deprived of oxygen
-The birth will proceed as normal if the presentation is vertex, but if the fetus presents by the breech and the midwife is not experienced in breech births she may need a doctor's assistance. • -The birth of the second twin should ideally be completed within 45 min of the first twin but, as long as there are no signs of fetal distress in the second twin
- it may be allowed to continue longer; if there are, the delivery must be expedited and the second twin may need to be born by caesarean section. • -A uterotonic drug (usually Syntocinon or Syntometrine) is usually given intramuscularly or intravenously, depending on local policy • -after the birth of the anterior shoulder as with a singleton pregnancy.
- This baby and cord are labelled as ‘twin two’. • - The time of birth and sex of child must be noted. • -The risk of asphyxia is greater for the second twin and the paediatric team may need to actively resuscitate this infant. • - may need to be transferred to the neonatal unit ,his mother should have a chance to see him first and, if at all possible be allowed a cuddle with him.
-Once the uterotonic drug has taken effect, controlled cord traction is applied to both cords simultaneously and the placentae delivered without delay. • - Emptying the uterus enables bleeding to be controlled and postpartum haemorrhage prevented. • -The placenta(e) should be examined and the number of amniotic sacs, chorions and placentae noted
-If the babies are of different sexes, they are dizygotic. If the placenta is monochorionic (MCDA), they must be monozygotic. • -If they are of the same sex and the placenta is dichorionic (DCDA), then further tests will be needed
-The umbilical cords should also be examined and the number of cord vessels and the presence of any abnormalities noted.