Download
1 / 15
150 likes | 493 Views
Khalid M. Al- Arfaj , MDFatemah Al- Shamlan , MD Mohammed Hantera , MD Financial Disclosure: NONE . Dammam University Dhahran Eye Specialist Hospital. Short Term Visual Outcomes Boston Keratoprosthesis Type I. INTRODUCTION.

E N D
Khalid M. Al-Arfaj, MDFatemahAl-Shamlan, MD Mohammed Hantera, MD Financial Disclosure: NONE Dammam University Dhahran Eye Specialist Hospital Short Term Visual Outcomes Boston Keratoprosthesis Type I
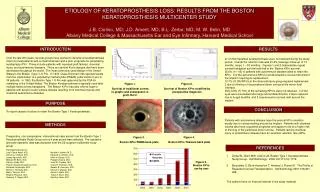
INTRODUCTION • Clinical experience with keratoplasty over the past century showed that patients with Stevens-Johnson syndrome (SJS), ocular cicatricialpemphigoid (OCP), chemical burns, stem cell deficiencies, and severe vascularization have an extremely poor prognosis.1 In addition, patients with repeated graft failures also have poor likelihood of successful subsequent corneal allo-grafting.2
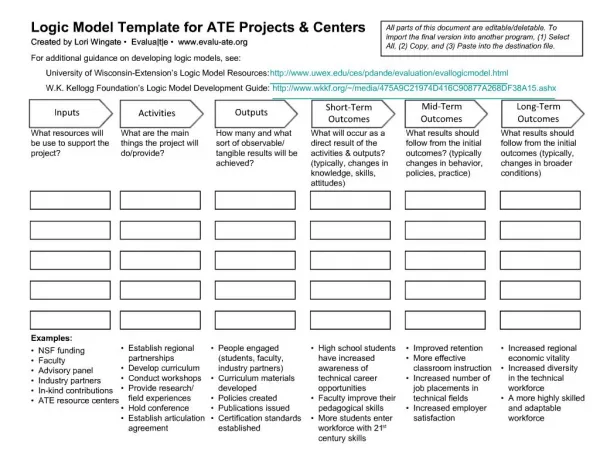
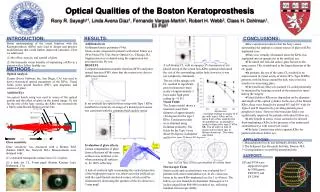
Boston Keratoprosthesis (Massachusetts Eye and Ear Infirmary, Boston, MA) is the most commonly used keratoprosthesis.3 • Our study was designed to evaluate the visual outcomes, complications and retention of threadless type I Boston KPro. The snap-onthreadless back plate facilitates easier intraoperative assembly and prevents any shredding of endothelium and descemet’s by the posterior plate screwing. To the best of our knowledge, such data has not been reported before in the Middle East.
There are 2 variants of the device. Type I, the more common variant, is a collar button-shaped device with front plate (diameter 5.5–7.0 mm),3 a central optical stem, and a back plate (available in 8.5 mm diameter adult size and 7.0 mm diameter paediatric size),4 with eight holes that facilitate the nutrition and hydration of the corneal graft.5, 6
PATIENTS AND METHODS • We undertook a retrospective analysis of 6 eyes of 6 patients (3 females and 3 males; age range: 48 to 72 years) who underwent Boston type I threadlesskeratoprosthesis implantation at a tertiary care eye hospital in Saudi Arabia by a single surgeon with similar surgical technique.
Surgical technique • Standard surgical technique as described by Dohlman and Barnes was followed.8 • Donor cornea was trephined with a 3 mm trephine and optical cylinder of the Kpro was passed through it. The back plate of the KPro was then snapped onto the stem with no rotating movement. • A titanium locking ring is finally snapped in place behind the back plate to prevent loosening of the back plate. • The graft prosthesis combination is then transferred to the patient’s trephined corneal opening and sutured with sixteen 10-0 monofilament nylon interrupted sutures.
Finally, a soft contact lens (Kontur lens; KonturKontact Lens Co., Hercules, CA), 16 mm diameter and 9.8 mm base curve, plano power, is placed as a bandage lens. • All patients received lifelong prophylactic antibiotics: guttmoxifloxacin 0.5% (Vigamox, Alcon Inc., Hunenberg, Switzerland), guttVacomycin fortified drops (25mg/ml) qid, gutt Prednisolone Acetate 1% (Predforte, Allergan, Inc. ,Irvine, CA, U.S.A.), and Tears Naturale Free (Alcon Inc., Hunenberg, Switzerland).
Conclusion • Careful follow-up for patients with severe ocular surface disease with Boston Kpro is crucial for the long-term success and survival of the procedure. • Boston Kpro has shown improved clinical results and decreasing complications. • It has promising results especially in the category of non autoimmune patients but continued innovations and clinical trials are needed.
References 1.Khan B, Dudenhoefer EJ, Dohlman CH. Keratoprosthesis: an update. CurrOpinOphthalmol 2001;12(4):282-287. 2.Dunlap K, Chak G, Aquavella JV, Myrowitz E, Utine CA, Akpek E. Short-term visual outcomes of Boston type 1 keratoprosthesis implantation. Ophthalmology 2010;117(4):687-692. 3.Ilhan-Sarac O, Akpek EK. Current concepts and techniques in keratoprosthesis. CurrOpinOphthalmol 2005;16(4):246-250. 4.Dohlman CH, Harissi-Dagher M. The Boston Keratoprosthesis: A New Threadless Design. Digital Journal of Opthalmology 2007 [Cited: August 05, 2010];13(3):[about 6 p.]. Available from: http://www.djo.harvard.edu/site.php?url=/physicians/oa/1055. 5.Dohlman CH, Dudenhoefer EJ, Khan BF, Morneault S. Protection of the ocular surface after keratoprosthesis surgery: the role of soft contact lenses. Clao J 2002;28(2):72-74. 6.Dudenhoefer EJ, Nouri M, Gipson IK, Baratz KH, Tisdale AS, Dryja TP, Abad JC, Dohlman CH. Histopathology of explanted collar button keratoprostheses: a clinicopathologic correlation. Cornea 2003;22(5):424-428. 7.Sayegh RR, Avena Diaz L, Vargas-Martin F, Webb RH, Dohlman CH, Peli E. Optical functional properties of the BostonvKeratoprosthesis. Invest Ophthalmol Vis Sci 2010;51(2):857-863 8.Dohlman CH, Barnes S MJ. keratoprosthesis. In: Krachmer JH, Mannis MJ, Holland EJ, eds. Cornea, 2nd ed. St Louis, MO: Mosby–Year Book Inc., 2005.