Download
1 / 23
400 likes | 674 Views
Female Hair Loss. By Sian Chess-Williams August 2011. Introduction. Hair History, Examination, Investigations. Different causes. Short Cases Summary. Hair. Hair follicle growth cycle: Anagen (growth phase) Catagen (involution phase) Telogen (shedding phase)

E N D
Female Hair Loss By Sian Chess-Williams August 2011
Introduction • Hair • History, Examination, Investigations. • Different causes. • Short Cases • Summary
Hair • Hair follicle growth cycle: • Anagen (growth phase) • Catagen (involution phase) • Telogen (shedding phase) Most hairs are in the anagen phase which lasts 3-5 years.
Hair loss Non scarring alopecia Scarring alopecia Due to a disorder within the scalp skin that causes permanent loss of the follicle. Causes shiny atrophic bald areas in the scalp which are devoid of follicular openings. • Due to a disorder of the hair follicle • The scalp looks normal
History • Onset • Sudden or gradual • Where was it noticed most • PMH (systemic disease, thyroid problems) • FH of hair loss. • Medication. • Dietary habits • Impact, hair routine. • Gynaecological / Obstetric history (menarche, menstrual, hormones, pregnancy, infertility) • Androgen excess
Examination • Examine the pattern and distribution of hair thinning. • Examine the scalp for any bald patches, scarring, erythema, or scaling. • Consider the pull test (only if personal experience allows). The technique is to tug a bundle of approximately 50–60 hairs firmly, but not forcibly, away from the scalp, sliding the fingers along the hair shaft. The test is positive if more than 10% of grasped hairs (around six hairs) are pulled away from the scalp. It indicates active hair shedding. • Look for features of hyperandrogenism, such as excessive facial and body hair (hirsutism), severe acne, and seborrhoea of scalp and skin.
Investigations • TFT • FBC • Ferritin • If androgen access (PCOS, androgen secreting tumours) consider: Free-androgen index test [FAI = total testosterone x 100 /sex hormone-binding globulin (SHBG)] & Prolactin level. • Combined hormonal contraception should be stopped 2 months before measuring this. • The measurements should be taken between 8-9am, ideally between the 2nd & 5th days of the menstrual cycle.
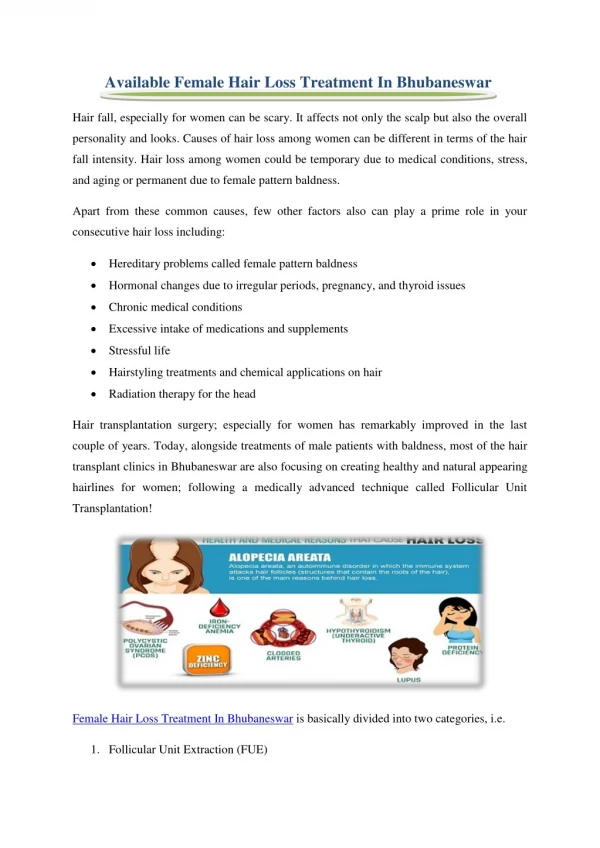
Causes: • Systemic disease (severe infection, thyroid dysfunction (hypo/hyper), endocrine disorders, iron deficiency, SLE, cancer) • Drugs (anabolic steroids, progestogens, antithyroid drugs, chemotherapy, antidepressants, anticoagulants, birth control pills, and hormonal treatments) • Extreme dietary habits & rapid weight loss. • Telogen effluvium • Alopecia areata • Androgenic alopecia • Ringworm (tineacapitis) • Traction alopecia (from hair being pulled back in styles like a ponytail or tight plaiting) • Hair fragility from chemical application (such as bleaching). • Scarring hair loss: Radiation, burns, shingles, teriary syphilis, lupus erythematosus, morphoea, lichen planus.
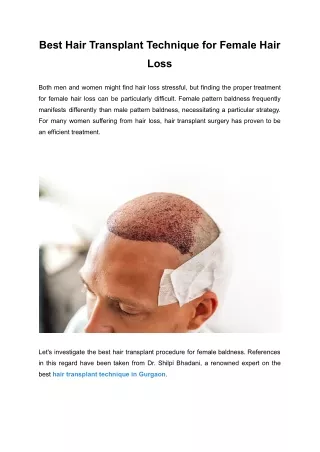
Androgenic alopecia • aka Female Pattern Hairloss (FPHL). • Most common type of non-scarring baldness. • Incidence is 5-10% pre-menopause & 20-30% post menopause. • History: androgen excess (hirsutism, acne, seborrhoea, virilization, menstrual irregularities, infertility, galactorrhoea, PCOS) • Women often though have normal hormone profiles & non other signs of excess androgens. • Typically there is slow progressive thinning in the density of hair at the crown and frontal scalp, and widening of the central parting with retention of the frontal hairline. • The pull test is usually negative in androgenetic alopecia, except in active periods where there may be a moderate degree of telogen hair shedding. • The onset is usually slowly progressive and hair loss is often diffuse. • Women tend not to develop total bald areas. Hair density often remains greatest over the occipital scalp. • Hair may be shampooed as frequently as desired without fear of worsening hair loss. • Local support groups or counselling may be of value if the woman requires psychological support
Androgenic alopecia management • Topical Minoxidil 2% solutionis the only drug licensed for use in female androgenetic alopecia. • Apply 1ml to the affected area(s) of hair loss on the scalp twice a day. • Allow hair to dry naturally. Wash your hands after use. • It is not prescribable on the NHS but can be bought over the counter or prescribed privately. • Hair loss will resume once treatment is stopped within 4 months, and this rebound shedding may be severe. • About 1 in 4 women report 'moderate' or more hair regrowth. • Hair regrowth may not be noticed for 4 months.
Telogen Effluvium • A pattern of diffuse hair loss that occurs about 3 months after childbirth or severe illness (severe infection, crash diets, major surgery), or may be precipitated by some medications. • The “stress” puts all the hairs into the telogen phase of hair shedding at the same time. • In the active phase, the “pull test” may be positive. Later, regrowth with tapered short hairs may be seen. • The hair fully recovers & the normal staggered hair growth / hair shedding cycle resumes.
Alopecia areata • Autoimmune, chronic inflammatory non-scarring disorder of hair growth. Often a genetic link (20% have a FH). • Lifetime prevalence 1.7%. • Clinical diagnosis. Often a circular bald patch with exclamation mark hairs (isolated short broken off hairs at the edge of a bald area is diagnostic). • May be associated with other organ-specific autoimmune disease. • Alopecia totalis (all head hair) is rarer & Alopecia universalis (all body) even more rare. • Prognosis: • 33% will have regrown in 6 months • 50% in 12 months • 33% will never recover. • Almost everyone who gets a first patch will do so again. • Poor prognosis: <10 yrs old, alopecia totalis, atopy, downs syndrome, nail dystrophy. (in 10% pitted or roughened)
Alopecia Areata Management • To treat or not to treat as 50% will recover without treatment • If significant hair loss, consider referral for treatment. • Intra-lesional corticosteroids – 1st line • Dithranol – 2nd line. • Topical immunotherapy • Topical super-potent steroids • Systemic corticosteroids • Minoxidil – most beneficial in preventing relapse.
Trichotillomania • a psychiatric condition in which people pull their hair out. It may be associated with obsessive-compulsive disorder and is more common in females than males. Hair loss is asymmetrical and has an unusual shape. Single or multiple areas can be affected, including eyebrows and eyelashes.
Case 1 • 26 year old lady with 1 month of diffuse hair loss. No FH. Given birth 10 weeks ago, periods now back to normal. On levothyroxine.
Case 2 • 40 year old lady with hair loss. Had patch of hair loss about 10 years ago which got better on its own by 1 year.
Case 3 • 54 year old lady, gradual hair loss for over a year. Normal periods thoughout life but went through menopause 2 years ago. Washes hair everyday, worried this caused it.
Female Hair Loss • Will come across frequently as a GP. • With structure to history & examination, we can clinically diagnose most, with blood test to confirm no other cause.
References • Clinical Knowledge Summaries • The GP Update Handbook Autumn 2010 • Oxford handbook of General Practice, second edition. • Kumar & Clark, Clinical Medicine, Fifth Edition.

![[Infographic] Female Hair Loss Facts and Statistics](https://cdn4.slideserve.com/7374511/slide1-dt.jpg)