Download
1 / 20
200 likes | 224 Views
Learn about Intensified Case Finding for TB among People Living with HIV, its challenges, tools, and recommendations based on the WHO presentation.

E N D
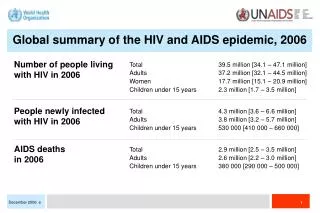
Living with HIV, Dying of TB Intensified TB case finding among people living with HIV Adapted from presentation by Colleen Daniels TB/HIV Advocacy Stop TB Department, WHO
Outline of presentation • What is intensified case finding? • Global implementation of TB case finding • Challenges • Conclusions
Intensified Case Finding (ICF) • Intensified TB case finding (ICF) is an activity, recommended by the World Health Organization (WHO), intended to detect possible TB cases as early as possible among people living with HIV • Screening for symptoms and signs of TB • + TB treatment • TB sputum smear • - IPT • ICF is the first step towards making a TB diagnosis.
Intensified Case Finding (ICF) • TB control programs generally rely on passive TB case finding • People living with HIV are at much greater risk of getting TB and if not treated soon enough, dying from it • often aggressive cases including hard-to-diagnose smear-negative or extrapulmonary disease. • ICF consists of using a simple questionnaire looking for the signs and symptoms of TB.
Percentage of PLHIV screened for TB in countries with 80% of the global burden, 2006.
Proportion of PLHIV screened and diagnosed with TB in selected countries, 2006 29% 8% 20% 31%
Symptoms and signs Adults (any of) 1. Cough (of any duration)? 2. Blood stained sputum? 3. Night sweats >2 weeks 4. Fever ? 5. Weight loss? 6. Chest pain? 7. Breathlessness? 8. Fatigue? 9. History of previous TB treatment? 10. History of close contact with a person confirmed to have TB? 11. Swellings in the neck, armpits or elsewhere? 12: Diarrhea for more than two weeks? Symptom and signs Children (any of) 1. Cough: (of any duration)? 2. Blood stained sputum? 3. Night sweats >2 weeks 4. Fever? Of any duration? 5. Weight loss? 6. Chest pain? 7. Fast Breathing? 8. Fatigue? 9. History of previous TB treatment? 10. History of close contact with a person confirmed to have TB? 11. Swellings in the neck, armpits or elsewhere? 12: Diarrhea for more than 2 weeks? 13. Failure to thrive? National screening strategy: Kenya
Any of the following Cough more than 3wks Weight loss Fever or night sweats Fatigue/tiredness Loss of appetite Lymph node enlargement National screening strategy: Malawi
Screening tools in countries • Screening tools vary from country to country • More and more non-specific constitutional symptoms and signs included in tools • Children are not addressed • Presence of nationally recommended screening tool does not always guarantee implementation
Challenge: implementation issues • Standardised screening tool needed? • Screening tool that can rule out active TB disease is needed and how best to link it with IPT? • Who administers the standard tool and where? • How often should it be administered? • Monitoring and evaluation- how should it be recorded and reported?
Review of some published evidence of TB screening strategies
Sensitivity= 95% Specificity= 10% Kimerling, et.al – Cambodia,2002IJTLD 2002; 6:988–994
Sensitivity= 91% Specificity= 59% Sensitivity= 59% Specificity= 76% Day, et. al. – South Africa, 2006IJTLD 2006: 10:523-529
Demissie, et.al. – EthiopiaWorld Lung Health Conference 2007 Abstract S11
Some Notes and Observations from available evidence • Sesitivity: Ability of the test to accurately diagnose the presence of disease. • Specificity: Ability of the test to accurately identify all people without the condition These are both measures of accuracy of a screening tool to identify a person with TB, the higher the Sensitivity and Specificity the more accurate the tool. • The accuracy of screening are generally inconsistent and dependent what types of screening questions are asked. Eg: the more the symptoms the greater the chances of detecting anyone with TB, but also the greater the chances of wrongly suspecting that people have TB when they don’t. • Chronic cough more than 2 or 3 wks alone looks insensitive predictor of TB in PLHIV • Role of CXR is not clear and inconsistent
Living with HIV, Dying of TB Conclusions • People with HIV have the right to ask for TB screening and diagnosis. • Check your country's progress in implementing the 12 collaborative activities and engage with the NTP and NAP to call for scale up (Global TB Report)
Conclusions • Mobilization by civil society urgently needed to scale up ICF. • Community driven to create demand • Educate – increase literacy in communities and at health care facilities • Work with joint TB/HIV national mechanisms to rapidly scale up • Engage in processes such as Global Fund CCMs • Demand creation • Myth busting - ensure that arguments about challenges to implementation are not a barrier (HIV experience) - Just do it!
Conclusions • Massive research efforts to develop the best and feasible screening tool are urgently needed • "TB dipstick test"- simple and rapid tool is crucial • Call for investment and increase in laboratory capacity and call for adequate referral systems • Recording and reporting