Download
1 / 1
10 likes | 75 Views
This study compares symptoms in HIV patients on EFV/FTC/TDF regimen with those on other antiretroviral therapies. It explores the association between symptoms, disease severity, adherence, and Health-Related Quality of Life (HRQoL) in these patients.

E N D
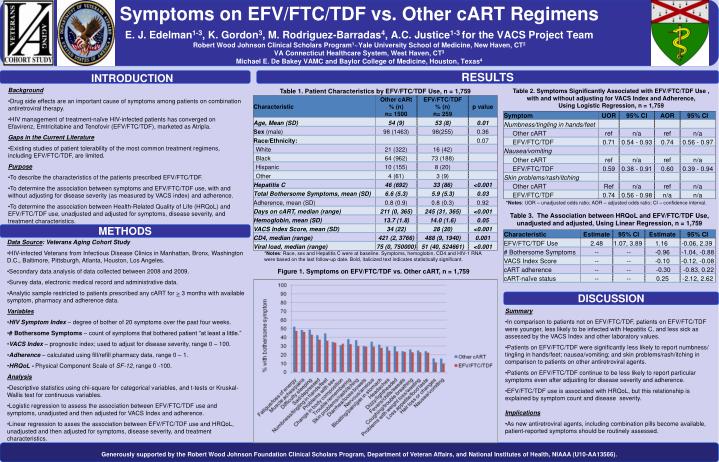
Symptoms on EFV/FTC/TDF vs. Other cART RegimensE. J. Edelman1-3, K. Gordon3, M. Rodriguez-Barradas4, A.C. Justice1-3 for the VACS Project TeamRobert Wood Johnson Clinical Scholars Program1~Yale University School of Medicine, New Haven, CT2VA Connecticut Healthcare System, West Haven, CT3Michael E. De Bakey VAMC and Baylor College of Medicine, Houston, Texas4 INTRODUCTION RESULTS • Background • Drug side effects are an important cause of symptoms among patients on combination antiretroviral therapy. • HIV management of treatment-naïve HIV-infected patients has converged on Efavirenz, Emtricitabine and Tenofovir (EFV/FTC/TDF), marketed as Atripla. • Gaps in the Current Literature • Existing studies of patient tolerability of the most common treatment regimens, including EFV/FTC/TDF, are limited. • Purpose • To describe the characteristics of the patients prescribed EFV/FTC/TDF. • To determine the association between symptoms and EFV/FTC/TDF use, with and without adjusting for disease severity (as measured by VACS index) and adherence. • To determine the association between Health-Related Quality of Life (HRQoL) and EFV/FTC/TDF use, unadjusted and adjusted for symptoms, disease severity, and treatment characteristics. Table 1. Patient Characteristics by EFV/FTC/TDF Use, n = 1,759 Table 2. Symptoms Significantly Associated with EFV/FTC/TDF Use , with and without adjusting for VACS Index and Adherence, Using Logistic Regression, n = 1,759 *Notes: UOR – unadjusted odds ratio; AOR – adjusted odds ratio; CI – confidence interval. Table 3. The Association between HRQoL and EFV/FTC/TDF Use, unadjusted and adjusted, Using Linear Regression, n = 1,759 METHODS • Data Source: Veterans Aging Cohort Study • HIV-infected Veterans from Infectious Disease Clinics in Manhattan, Bronx, Washington D.C., Baltimore, Pittsburgh, Atlanta, Houston, Los Angeles. • Secondary data analysis of data collected between 2008 and 2009. • Survey data, electronic medical record and administrative data. • Analytic sample restricted to patients prescribed any cART for > 3 months with available symptom, pharmacy and adherence data. • Variables • HIV Symptom Index – degree of bother of 20 symptoms over the past four weeks. • # Bothersome Symptoms – count of symptoms that bothered patient “at least a little.” • VACS Index – prognostic index; used to adjust for disease severity, range 0 – 100. • Adherence – calculated using fill/refill pharmacy data, range 0 – 1. • HRQoL - Physical Component Scale of SF-12, range 0 -100. • Analysis • Descriptive statistics using chi-square for categorical variables, and t-tests or Kruskal-Wallis test for continuous variables. • Logistic regression to assess the association between EFV/FTC/TDF use and symptoms, unadjusted and then adjusted for VACS Index and adherence. • Linear regression to asses the association between EFV/FTC/TDF use and HRQoL, unadjusted and then adjusted for symptoms, disease severity, and treatment characteristics. *Notes: Race, sex and Hepatitis C were at baseline. Symptoms, hemoglobin, CD4 and HIV-1 RNA were based on the last follow-up date. Bold, italicized text indicates statistically significant. Figure 1. Symptoms on EFV/FTC/TDF vs. Other cART, n = 1,759 DISCUSSION • Summary • In comparison to patients not on EFV/FTC/TDF, patients on EFV/FTC/TDF were younger, less likely to be infected with Hepatitis C, and less sick as assessed by the VACS Index and other laboratory values. • Patients on EFV/FTC/TDF were significantly less likely to report numbness/ tingling in hands/feet; nausea/vomiting; and skin problems/rash/itching in comparison to patients on other antiretroviral agents. • Patients on EFV/FTC/TDF continue to be less likely to report particular symptoms even after adjusting for disease severity and adherence. • EFV/FTC/TDF use is associated with HRQoL, but this relationship is explained by symptom count and disease severity. • Implications • As new antiretroviral agents, including combination pills become available, patient-reported symptoms should be routinely assessed. Generously supported by the Robert Wood Johnson Foundation Clinical Scholars Program, Department of Veteran Affairs, and National Institutes of Health, NIAAA (U10-AA13566).






