Download
1 / 17
480 likes | 1.58k Views
Clinical decision making. Carl Thompson UK, Centre for Evidence Based Nursing Editor, Evidence Based Nursing www.ebn.bmj.com. This session. Integrating research evidence with preferences and contextual information The ways people think and make choices

E N D
Clinical decision making Carl Thompson UK, Centre for Evidence Based Nursing Editor, Evidence Based Nursing www.ebn.bmj.com
This session • Integrating research evidence with preferences and contextual information • The ways people think and make choices • When should intuition and more structured approaches be used? • What’s right and wrong with clinical experience? • Tools and techniques: decision analysis, cognitive approaches
How do nurses (and doctors) think they think? • Make sense of multiple cues • Diagnose or assess • Treat or intervene • Evaluate progress • Treat some more if needed • Errr… start again…
The theory – cognitive continuum Hamm,R (1988) in Dowie & Elstein, Clinical Judgement and decision making, Cambridge University Press
Heuristics and Bias Daniel Kahneman and Amos Tversky (d. 1996) Tversky and Kahneman, Judgment Under Uncertainty: Heuristics and Biases, Science (1974), Vol. 185, pp 1124-1131
The Need to Assess Probabilities • People need to make decisions constantly: diagnosis and therapy • Thus, people need to assess probabilities to classify objects or predict various values, such as p (DISEASE|SYMPTOMS) • People employ heuristics to assess probabilities • heuristics lead to significant biases, CONSISTENTLY • This observation leads to a descriptive, rather than a normative, theory of human probability assessment
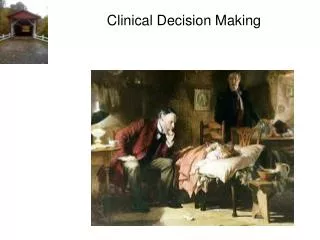
Experience: A problem of perceptionSlide from Slawson, Shaughnessy, Becker, 1999. Do you see the Dalmation in the picture? Moral: Clinical experience sometimes helps see, sometimes prevents seeing the right picture Now that you see it, can you try tonotsee it? Moral: Experience can result in ideas that are difficult to change
Then one can see the pattern where before it had been confusing.
Time and nursing decisions • Once every 30 seconds in critical care (Bucknall, 2000) • Circa 50 decisions every 8 hour shift in Medical Admissions (Thompson et al. 2001 – 2005) • 5 judgement or decision challenges per consult for health visitors.
Remember uncertainty? • How do we normally respond? • Experiential/internal knowledge • Very limited textual information use and for certain kinds of decisions (British National Formulary and local protocols) • 90 hours of primary care = 1 telephone call • 180 hours of acute care (1080 decisions) = local protocols x4 times, BNF x50 times). • ‘sophistication’ and technology doesn’t matter (Randell et al. 2007). • Demography and biography poor predictors of use
The five classic decision pitfalls • Representativeness and base rate neglect • Availability • Overconfidence • Confirmation • Illusory correlations
What can we do? • Think about decision structure, time & visibility • Be aware of base rates • Consider whether information is truly relevant and not just salient • Seek reasons why you may be wrong and entertain alternatives • Ask questions that may disprove, rather than confirm, your current hº • You are wrong more often than you think