Download
1 / 2
30 likes | 190 Views
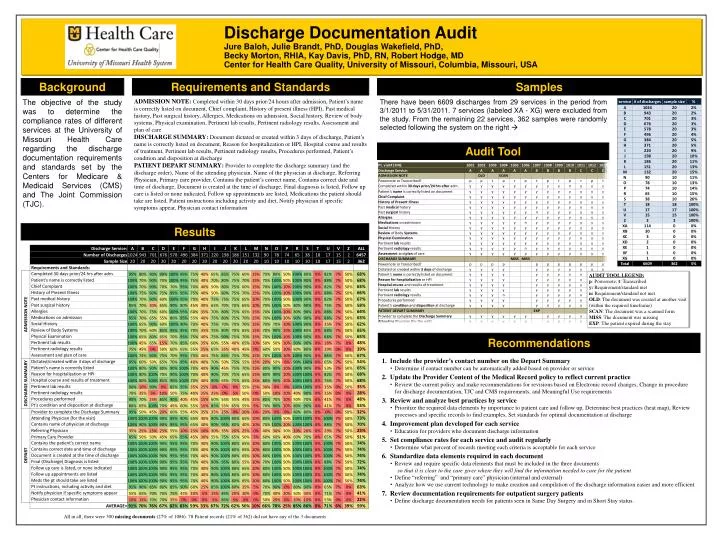
Discharge Documentation Audit Jure Baloh, Julie Brandt, PhD, Douglas Wakefield, PhD, Becky Morton, RHIA, Kay Davis, PhD, RN, Robert Hodge, MD Center for Health Care Quality, University of Missouri, Columbia, Missouri, USA. Samples. Background. Requirements and Standards.

E N D
Discharge Documentation Audit Jure Baloh, Julie Brandt, PhD, Douglas Wakefield, PhD, Becky Morton, RHIA, Kay Davis, PhD, RN, Robert Hodge, MD Center for Health Care Quality, University of Missouri, Columbia, Missouri, USA Samples Background Requirements and Standards ADMISSION NOTE: Completed within 30 days prior/24 hours after admission, Patient’s name is correctly listed on document, Chief complaint, History of present illness (HPI), Past medical history, Past surgical history, Allergies, Medications on admission, Social history, Review of body systems, Physical examination, Pertinent lab results, Pertinent radiology results, Assessment and plan of care DISCHARGE SUMMARY: Document dictated or created within 3 days of discharge, Patient’s name is correctly listed on document, Reason for hospitalization or HPI, Hospital course and results of treatment, Pertinent lab results, Pertinent radiology results, Procedures performed, Patient’s condition and disposition at discharge PATIENT DEPART SUMMARY: Provider to complete the discharge summary (and the discharge order), Name of the attending physician, Name of the physician at discharge, Referring Physician, Primary care provider, Contains the patient’s correct name, Contains correct date and time of discharge, Document is created at the time of discharge, Final diagnosis is listed, Follow up care is listed or none indicated, Follow up appointments are listed, Medications the patient should take are listed, Patient instructions including activity and diet, Notify physician if specific symptoms appear, Physician contact information The objective of the study was to determine the compliance rates of different services at the University of Missouri Health Care regarding the discharge documentation requirements and standards set by the Centers for Medicare & Medicaid Services (CMS) and The Joint Commission (TJC). There have been 6609 discharges from 29 services in the period from 3/1/2011 to 5/31/2011. 7 services (labeled XA - XG) were excluded from the study. From the remaining 22 services, 362 samples were randomly selected following the system on the right Audit Tool Results AUDIT TOOL LEGEND: p: Powernote; t: Transcribed y: Requirement/standard met n: Requirement/standard not met OLD: The document was created at another visit (within the required timeframe) SCAN: The document was a scanned form MISS: The document was missing EXP: The patient expired during the stay Recommendations • 1. Include the provider’s contact number on the Depart Summary • Determine if contact number can be automatically added based on provider or service • 2. Update the Provider Content of the Medical Record policy to reflect current practice • Review the current policy and make recommendations for revisions based on Electronic record changes, Change in procedure for discharge documentation, TJC and CMS requirements, and Meaningful Use requirements • 3. Review and analyze best practices by service • Prioritize the required data elements by importance to patient care and follow up, Determine best practices (heat map), Review processes and specific records to find examples, Set standards for optimal documentation at discharge • 4. Improvement plan developed for each service • Education for providers who document discharge information • 5. Set compliance rates for each service and audit regularly • Determine what percent of records meeting each criteria is acceptable for each service • 6. Standardize data elements required in each document • Review and require specific data elements that must be included in the three documents • so that it is clear to the care giver where they will find the information needed to care for the patient • Define “referring” and “primary care” physician (internal and external) • Analyze how we use current technology to make creation and compilation of the discharge information easier and more efficient • 7. Review documentation requirements for outpatient surgery patients • Define discharge documentation needs for patients seen in Same Day Surgery and in Short Stay status. • All in all, there were 300 missing documents (27% of 1086). 78 Patient records (21% of 362) did not have any of the 3 documents