Download
1 / 44
450 likes | 531 Views
Learn about the key considerations in maintaining and restoring dental health post endodontic treatment to promote healing. Understand the importance of coronal restoration and material choices for optimal outcomes. Explore clinical guidelines and restoration options.

E N D
Restorative considerations for endodontically treated teeth. ADA Meeting 19 July 2011 www.endodonticpractice.co.nz
Endodontics • The branch of dentistry that deals with maintaining healthy dental pulp in a state of health and the treatment of diseased dental pulp to promote healing and restoring the health of the tooth and the surrounding peri-radicular tissues to maintain the function and aesthetics of the teeth.
The Consultation - History - Exam - Diagnosis - Treatment plan - Treatment - Recall
The Plan Coronal Restoration - Remaining tooth structure - Periodontium - Strategic importance - Occlusion - Material(s) - Additional Retention - Nayyar technique - Posts? - PINS Root Canal Treatment - Non-surgical - Surgical
Posts Posts DO NOT strengthen root filled tooth They retain the core NO POST is the best option However……….
Posts • Type - Prefabricated not cast post
Posts • Shape – Parallel sided not tapered
Posts • Length – Long not short The Crowbar Effect
Posts • Diameter – Debatable α material
Posts • Material – Rigid and not flexible Gold, fibre such as carbon, glass, or even zirconia, or stainless steel, or titanium
Posts • Design – Serrated (not smooth or screw type) Screw Serrated Smooth
Posts • Cement – Type and amount Whatever type of cement that is used for the post it t must fit loosely in the canal. If you are a getting a tug back with your post, you have a problem.
Clinical Guidelines • Prefabricated • Long • Thick • Serrated • Parrallel • Rigid • Cement
Final Restoration/Core www.endodonticpractice.co.nz
Direct restoration • Amalgam • Advantages • - Proven track record • - Quick and easy to place • - Relatively Inexpensive • - Good coronal seal • Disadvantages • - Mercury • - Colour • - Does not bond to teeth • - Require retentive features
Direct restoration • Composite • Disadvantages • - Technique sensitive • - Coronal leakage • Advantages • - Matches tooth colour • - Less toxic • - Minimal preparation • - Bonds to teeth
Direct restoration • Glass Ionomer • Disadvantages • - Technique sensitive • - Weak • Advantages • - Matches tooth colour • - Less toxic • - Minimal preparation • - Moisture tolerant • - Releases flouride
In-direct restoration • Indirect CAD/CAM – CD4, Cerec • Advantages • - Matches tooth colour • - Less toxic • - Quick turn-around • - Bonds to teeth • Disadvantages • - Technique sensitive • - Brittle • - Cost - set up • - patients
In-direct restoration • Indirect lab based – Gold, PFM, PJC, Zirconia • Advantages • - Matches tooth colour • - Less toxic • - Good seal • - Restores tooth resistance • Disadvantages • - Time consuming • - Brittle – (Porcelain) • -Cost • - Delayed
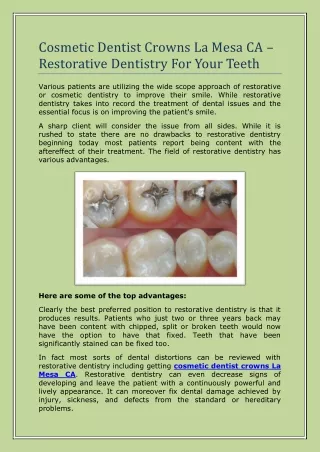
A virgin tooth is prestressed where the cusps are in constant tension pushing towards each other to allow for the flexing occlusal forces. • Occlusalfilling – 20 %. I will happily replace this with amalgam or composite. • MO or DO – 40 % I would restore them with amalgam or composite. However as soon as you roughly lose just over 2/3(M-D) x 1/3 (B-L) of the tooth I would seriously consider cusp capping with amalgam or composite • MOD – 60 % At this stage, I will do a full coverage restoration with amalgam or composite • If a cusp is missing then the ability to withstand fracture reduces even further. • When restoring a tooth, one must look at the remaning tooth structure and then decide what filling they will do. This is the primary determining factor. • The aim of the game to restore the tooth to as close to its original state.
Do all root filled teeth require crowns? • The routine use of posts and cores in anterior teeth is not required unless there is gross loss of coronal tooth structure. In fact there is lesser leakage with a bonded composite that a post core and crown. If you are going to make a veneer, you are better off making a crown. Generally too much tooth structure is lost to make a nice veneer so crown the tooth especially if it is heavily filled • Root canal treated posterior teeth, usually needs a crown when they are cusp capped. As a general rule, It can increase the chances of success by 6-11 fold. • In any case the core material that is used does not matter if there is sufficient tooth structure to provide a ferrule effect.
The Ferrule When using a core build up in either anterior or posterior teeth, ideally there must be at least 2 mm of sound tooth structure above the free gingival margin for the placement of a crown. This is the ferrule. This increases the resistance of teeth to fracture and also allows for the margins from getting plaque accumulation and subsequent secondary decay. 1mm ferrule double the resistance to fracture. Uneven ferrule is better than no Ferrule. So don’t pick up that bur and trim the last remaining millimetre of supra-gingival tooth just so that your cast post is easier to fit.
Crown Lengthening Surgery • 1.0 mm cemetal-fibrous interface, • 1.0 mm epithelial attachment, • 1.0 mm sulcus • 1.0 mm finishing margin = 4.0 mm above crestal bone Orthodontic extrusion is better than CLS
How long before a crown • Review in 6 months to check for healing. If no change. Review in another six months. • Crown when healing visible at the recall. • If crowning will reduce the chances of leakage such post core crown for anteriors. Crown immediately after RCT.
The Coronal Seal The coronal seal is NO more important than the root filling itself. Coronal seal Adequate root filling
Clinical Guidelines • Timing of final restoration • Tooth fracture prior to final restoration; • Inadequate final restoration • lacks ideal marginal integrity • forces of occlusalfunction • deterioration • Recurrent decay
Pathway to success • Correct diagnosis www.endodonticpractice.co.nz
Pathway to success • Rubber dam isolation www.endodonticpractice.co.nz
Pathway to success • Adequate Access
MB 2 is Not a Myth!! Pathway to success • Locate all the canals www.endodonticpractice.co.nz
Pathway to success • Thorough chemo-mechanical preparation
Pathway to success • Well constructed provisional restoration
Pathway to success • Unidentified Iatrogenic damage Perforation www.endodonticpractice.co.nz
Pathway to success • Produce an acceptable root filling and construct a good coronal seal
Outcomes • Favourable - Healing - Pre-operative PA area 73%-97% - More than 2 roots 84% - No pre-operative PA area 88%-97% - Single rooted teeth 93% • Overall • Healing 41% - 86%
Conclusion • Each case must be treated on its own merit • There is no “recipe” to ensure success • Ensure correct informed consent • Refer if unsure “Do or do not... there is no try.” – Yoda www.endodonticpractice.co.nz