Download
1 / 17
180 likes | 374 Views
When Laboratory Testing Turns Against Us : Human Anti-Mouse Antibody (HAMA) Interference with TSH and PTH Assays. Sadaf A. Farooqi , MD. Disclosure. No conflict of interest for the authors Sadaf Farooqi , MD Justin Moore, MD Rami Mortada , MD

E N D
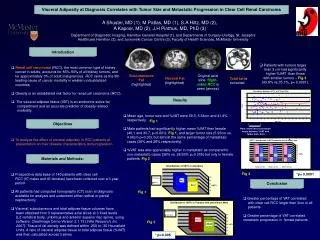
When Laboratory Testing Turns Against Us:Human Anti-Mouse Antibody (HAMA) Interference with TSH and PTH Assays Sadaf A. Farooqi, MD
Disclosure No conflict of interest for the authors • SadafFarooqi, MD • Justin Moore, MD • RamiMortada, MD • No financial incentives are involved in this presentation
Introduction • Heterophile antibodies, like Human Anti-Mouse Antibody (HAMA) can lead to falsely elevated levels of TSH and PTH • This occurs in specific “sandwich” immunoassays, leading to expensive investigations and unnecessary treatments
Case Presentation Case 1 • 24 yr. old ♀ with Hashimoto’s disease • Wide fluctuation in her TSH levels (76 to 276 mU/L) normal 0.5-5.0mU/L • Multiple escalations of her thyroid hormone dosage lead to a hospitalization for tachycardia • HAMA - 600ng/ml • Levothyroxine replacement was reduced to a weight-based dose (~1.6 mcg/kg/day) • Free Thyroxine level was used for subsequent dose adjustment
Case 2 • 78 yr. old ♀with CKD presented with secondary hyperparathyroidism and widely labile PTH levels over one year (60-899 pg/ml; normal 10-65 pg/ml) • Serum Calcium and vitamin D levels unremarkable • Negative extensive evaluation, including a negative Sestamibi scan • HAMA titer 800ng/ml • Placed on activated vitamin D commensurate with her level of renal function • Subsequently felt well and no further workup or management was undertaken
Human Anti-Mouse Antibodies • Most commonly encountered Heterophile Antibody • 10% of the population may have HAMA which can interfere with immunoassays results
Hetrophile Antibodies HETROPHILE ANTIBODY
Human Anti-Mouse Antibodies • HAMA have broad reactivity with antibodies of other animal species which are often source of assays antibody • They can create both false positive and false negative results
False Positive From Interfering HeterophileAntibody LABEL ANTIBODY NO ANYLATE CAPTURE ANTIBODY HETEROHILE ANTIBODY
Other Tests Affected By Heterophile Antibodies • Tumor markers: CA 19-9, CEA, AFP • PSA • Troponin I • HCG • Hepatitis • Drug levels
Neutralizing The Effect Of HAMA Strategies • Repeat test with different assay • HAMA/Heterophile blocking reagents • Serial dilutions • Nonspecific antibody-blocking tubes • Some commercial kits detect HAMA-positive patient samples
What Should A Clinician Do? • Consider HeterophileAntibody interference if there is a discrepancy between clinical presentation and laboratory values • Clinicians should be aware of this type of interference in routine immunoassays • Document exposureto drugs and screen patients
What Clinical Labs Should Do? • Identify samples-dilution, blocking studies • HAMA assays • Encourage manufactures to make more effective blockers • Communicate with physicians the limitations of methodology
References Baskin HJ, Cobin RH, Duick DS, et al. AACE thyroid guidelines. EndocrPract 2002;8:457-69. Sapin R, Agin A, Gasser F. Misleading high thyrotropin results obtained with a two-site immunometric assay involving a chimeric antibody. ClinChem 2004;50:946-8. Baskin H J, Cobin R H, Duick D S. et al AACE thyroid guidelines. EndocrPract 2002. 8457–469.469. Hollowell J G, Staehling N W, Flanders W D. et al Serum TSH, T4 and thyroid antibodies in the United States population(1988–1994): National Health and Examination Survey (NHANES 3). J ClinEndocrinolMetab 2002. 87489–499.499. Cooper D S. Clinical practice: subclinical hypothyroidism. N Engl J Med 2001. 345260–265.265.