Download
1 / 16
160 likes | 411 Views
Cryptococcal meningitis and patients issue on antretroviral era in HIV-infected adults in West Africa. Ouattara SI, Diafouka-Pratt K, Doumbia A Mossou C, Kouakou G, Ehui E, Tanon A, Eholié SP, Kakou A, Aoussi E,Bissagnene E

E N D
Cryptococcal meningitis and patients issue on antretroviral era in HIV-infected adults in West Africa Ouattara SI, Diafouka-Pratt K, Doumbia A Mossou C, Kouakou G, Ehui E, Tanon A, Eholié SP, Kakou A, Aoussi E,Bissagnene E Service des Maladies infectieuses du CHU de Treichville ,Côte d’Ivoire
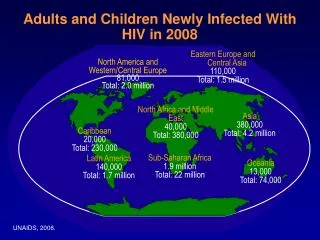
Introduction * 600.000 deaths /year linked to cryptococcal meningitis(CM) (4th cause of deaths due to infectious deseases on Subsaharan africa). * Initial mortality on the first 10 weeks vary 10-25% in developped countries opposed resources-limited settings 60-70% . * Sub-Saharan Africa , specially in Côte d’Ivoire, CM treated by Amphotericin B and/or fluconazole * Describe frequency , diagnosis and prognosis characteristic of this sever fungal during the last six years in larg access of ARV .
Objectives • General objective: • Describe epidemiological, clinical, paraclinical, therapeutic and evolutive characteristics of cryptococcal meningitis * Specifics objectives -Describe socio- demographics characteristics of the patients - Describe clinical and biological aspects of CM - Precise the issue of patients ;
Patients and methods (1) * Study: Retrospective study conducted at Clinical Infectious diseases of Treichville University Hospital on files of patients hospitalized for CM during 01 January 2005 to 31 december 2010 *Inclusion criteria HIV-infected patients ≥18 years CM confirmed by a CSF (India ink stain ,Cr Ag positive , fungal culture positive for Cryptococcus neoformans ) *collection’s data (card index-investigation) socio-demographic, clinical, biological, therapeutic characteristic and issue data . *Treatment :Antifungal +lumbar puncture discharge 2 times a week (20-30 CC) if intense headeache
Patients and methods (2) • Primary outcomes measure : letality and antifungal tolerance (adverse events grade III-IV) • Secondary outcome measure: Frequency of CM during the last six years *statistical analysis: Epi-Info 6.0. * Research of factors associated with death :univariate analysis (p<0.05)
General data Patients hospitalized N= 3836 . Cryptococcal meningitis N=104 (2,7%) HIV(-) patients non included N=4(0.1%) HIV(+) patients included N=100(2,6%)
Baseline characteristics of the study population variable number (N=100) Pourcentage(%) *Age (mean ,range ) 35[20-60] - *Gender Male 55 55 Female 45 45 *HIV type HIV1 95 95 HIV2 5 5 *NADIR CD4 (mean,range) 81[ 10-120] - *HAART ARV(+) 39 39 ARV(-) 61 61
Clinical characteristics Number Pourcentage(%) N=100 *Mean hospitalisation delay 5,4(3-17 ) - *Mode beginning -Subacute 81 81 -Acute 19 19 *functional signs -Fever 80 80 -Headeache 71 71 -conscienciousness altered 55 55 -convulsions 6 6 *Examination -Meningoencephalitis 61 61 -Meningitis 39 39
Paraclinics characteristics Number n=100 Pourcentage(%) *CSF macroscopic aspect Clear 71 71 Trouble 29 29 *Cytology Cells/mm3 (mean,range ) 112(1-1141) - *Biochemistry Hyper proteinorachy 92 92 Hypoglycorachy 92 92 hypochlorurorachy 92 92
Données sur les effets secondaires Data on tolerance and the patients issue Deads:43 (43%) survivors:57 (57%) CM-IRIS:9 cases Adverse events:205 Adverse events Grade III-IV:(n=49 ,23,9%) (33patients/100) Events Adverse events grade III-IV Pourcentage N=49 Anemia 14 28.5 Hypertransaminasemia 10 20.4 Thrombopenia 08 16.3 Hypokaliemia 07 14.2 Leucopenia 06 12.2 Neutropenia 02 04 Hyponatremia 01 02 Hypercreatininemia 01 02
Factors associated with death of CM Deaths n=43(%) survivors n=57(%) P *Gender 0.5 male 22(51,1) 33(57,9) Female 21(48,8) 24(42,1) *Delay hospitalisation 0.15 ≤48h 8(18,6) 5(8,8) >48h 35(81,4) 52(91,2) *Meningoencephalitis <0.01 yes 31(72,1) 23(40,3) No 12(27,9) 34(59,7) *Coma 0.02 ≤9 10(24,2) 3(6,4) >9 33(75,8) 54(93,6)
Factors associated with death of CM Décès n=43 Vivants n=57 P Cytorachy 0.40 ≤100 32(74,4) 38( 66,6) >100 11(25,6) 19(33,4) Lumbar puncture discha rge0.0002 yes 12(27.9) 37(69.8) No 31(72.1) 20(30.2) ARV 0.02 Yes 11(25,6) 28(49,1) No 32(74,4) 29(50,9) CD4≤100/mm3 26 (60,5) 39(68,4) 0.41 CD4>100/mm3 17(39,5) 18(31,6)
Comments *Clinical symptomatology dominated by meningoencephalitis symptoms is similar to the former series 71%(Souamaré,2005) ,80.5%( Bissagnene E,1994) *Emergency of CM -IRIS form in our study like the over study :17% ( Bicanic T,2009 ) *Lethality lower than the previous studies 80%( Millogo,2003) 71 %(SoumaréM,2005) 86,5% ( Bissagnene E,1994) *Tendencies which appeared on the associated factors associated witch deaths in univariate analysis was meningoencephalitis,coma , no ARV treatment , no lumbar puncture discharge
Conclusion * In spite of advent of ARV, cryptococcal meningitis is frequent and severe opportunistic infection of central nervous system in HIV-infected persons in Côte d’Ivoire * Improvement of the prognosis of this fungal is reinforced by the necessity of the lumbar puncture discharge and the early treatment of CM * Reinforce accessibility, the availability of the fluconazole and training of medical staff to the new therapeutic strategies of the CM necessary