Download

1 / 56
580 likes | 670 Views
DRUG RECEPTORS AND PHARMACODYNAMICS. PAUL EHRLICH 1845-1945 Drugs cannot act unless they are bound to receptors. PROTEIN TARGETS FOR DRUG BINDING. 4 main kinds of regulatory protein are commonly involved as primary drug targets Receptors Enzymes methotrexate-dihydrofolate reductase

E N D
PAUL EHRLICH 1845-1945 Drugs cannot act unless they are bound to receptors
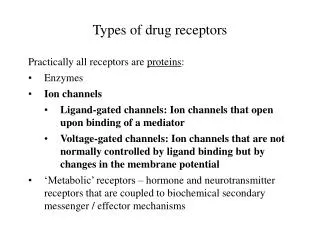
PROTEIN TARGETS FOR DRUG BINDING 4 main kinds of regulatory protein are commonly involved as primary drug targets • Receptors • Enzymes methotrexate-dihydrofolate reductase • Carrier molecules (transporters) (SSRI, TCA) • Ion channels local anesthetics-voltage sensitive Na channel
Pharmacodynamics Is what the drug does to the body. Interaction of drugs with cellular proteins, such as receptors or enzymes, to control changes in physiological function of particular organs. • Drug-Receptor Interactions • Binding • Dose-Response • Effect • Signal Transduction • Mechanism of action, Pathways
PHARMACODYNAMICS 2 • Receptors largely determine the quantitative relations between dose or concentration of drug and pharmacologic effects • Receptors are responsible for selectivity of drug action, the molecular size, shape and electrical charge of a drug determine its binding characteristics • Receptors mediate the actions of both pharmacologic agonists and antagonists
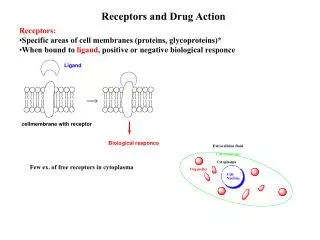
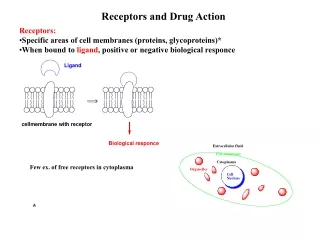
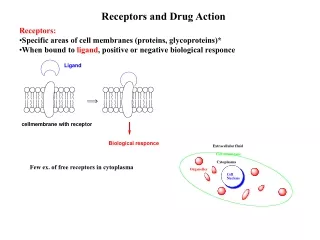
Drug receptor • A protein macromolecule produced by the body that was designed by nature to interact with an endogenous molecule (ligand), but which will also interact with a drug molecule, if it has the correct chemical structure
Levels of protein structure Primary→ sequence of aa that make up the pp chain Secondary →interaction of + charged H atoms with – charges O atoms on C from the same polypeptide chain Tertiary → interaction of aa that are relatively far apart on the protein backbone Quaternary → binding interaction among 2 or more independent protein subunits
Some receptor characteristics… • Ability to recognize specific molecular shapes: only a limited group of neurochemicals or drugs can bind to initiate a cellular response
Endogenous compounds act on their receptors Neurotransmitter Neuropeptides Hormones Ions
Best fit -- highest affinity Some fit; no cellular effect; block receptor preventing its activation by drug or neurochemical or hormone The ability of a drug to activate a receptor and generate a cellular response is its efficacy
Some receptor characteristics… Binding of ligand is only temporary Ligand binding produces physical changes in protein conformation, initiating intracellular changes that ultimately generates behavioral effects. Receptors have a life cycle (as other proteins do). Receptors can be modified in numbers (long-term regulation) and in sensitivity. • Receptors can up-regulate: increase in numbers (chronic absence of agonist) • Down-regulate: decrease in numbers (chronic presence of agonist)
PHARMACODYNAMICS AGONISTS & ANTAGONISTS • Receptors mediate the actions of both pharmacologic agonists and antagonists. Some drugs and many natural ligands such as hormones and neurotransmitters activate the receptor to signal as a direct result of binding to it. Agonists (Full agonists, Partial agonists, Inverse agonists) Antagonists bind to receptors but do not activate generation of a signal, they interfere with the ability of an agonist to activate the receptor.
There are 3 types of agonist... • Full agonist: Produces the maximal responce • Partial agonist (agonist-antagonist or mixed agonist-antagonist):produces the submaximal responce *In the presence of full agonist, a partial agonist will act like an antagonist because it prevents the full agonist to bind the receptor
An antagonist occupies but does not activate the drug receptor
Types of drug antagonism • chemical antagonism (interaction in solution) • pharmacokinetic antagonism (one drug affecting the absorption, metabolism or excretion of the other) • competitive antagonism (both drugs binding to the same receptors); the antagonism may be reversible or irreversible • interruption of receptor-effector linkage • physiological antagonism (two agents producing opposing physiological effects)
0 0
BINDING WITH RECEPTORS BONDS • Ionic bonds +++ • Hydrogen bonds ++ • Dispersion forces (Van der Waals) + • Covalent bonds ++++
Inhibition caused by reversible antagonist overcome by adequate concentration of agonist at receptor site Reversible antagonist Agonist RESPONSE
Irreversible antagonists permanently occupy (bond covalently) to their receptors
Dose-response relationships • The relationship between the concentration of drug at the receptor site and the magnitude of the response is called the dose-response relationship • Depending on the purpose of the the studies, this relatioship can be described in terms of a graded (continous) response or a quantal (all-or-none) response
graded dose-response relationship • In this relationship; percentage of a maximal response is plotted against the log dose of the drug • Illustrates the relatioship between drug dose, receptor occupancy and the magnitude of the resulting physiologic effect • It follows from receptor theory that the maximal response to a drug occurs when all receptors that can be occupied by that drug
Dose-response (dose-effect) curve Half maximal response indicates that 50% of the reseptors are occupied Maximal response indicates that, all receptors are occupied by drug EC 50 Median effective dose
drug efficacy • The ability of a drug to elicit a maximal response • Also called intrinsic activity of a drug Therapeutic efficacy, or effectiveness, is the capacity of a drug to produce an effect and refers to the maximum such effect. For example, if drug A can produce a therapeutic effect that cannot be obtained with drug B, however much of drug B is given, then drug A has the higher therapeutic efficacy. Differences in therapeutic efficacy are of great clinical importance.
RELATION BETWEEN DRUG CONCENTRATION AND RESPONSE A agonist response in the absence of an antagonist B low concentration antagonist C larger concentration of antagonist D and E spare receptors have been used up
quantal dose-response relationship • The response elicited with each dose of a drug is described in terms of the cumulative percentage subjects exhibiting a defined all-or-none effect and is plotted against the log dose of the drug • (prevention of convulsions, arrhythmia or death,relief of headache)
dose-response curves % of population tested
ED50: median effective dose • ED50 (median effective dose): • The dose of a drug that produces a specified, desired effect in 50% of the animal population tested
Quantal dose-response relationships. The dose-response curves for a therapeutic effect (sleep) and a toxic effect (death) of a drug are compared. The ratio of the LD50 to the ED50 is the therapeutic index. The ratio of the LD1 to the ED99 is the certain safety factor. ED = effective dose; and LD = lethal dose.
Toxic levels Drug plasma concen-tration Therapeutic levels Subtherapeutic levels
Therapeutic index (TI) TI = TD 50 ED50 The ratio of the dose producing a specified toxic effect in 50% of the test population (TD50)to the dose producing a specified desired effect in 50% of the test population (ED50)