Download
1 / 36
360 likes | 375 Views
Lymph Node Ratio Predicts for Survival in Gastric Cancer; A SEER Database Analysis. George W. Dombi, PhD 1 and Ravi Shridhar, MD-PhD 2 1 Epidemiology Division and 2 Gershenson Radiation Oncology Center Barbara Ann Karmanos Cancer Institute Detroit Medical Center Wayne State University

E N D
Lymph Node Ratio Predicts for Survival in Gastric Cancer; A SEER Database Analysis George W. Dombi, PhD1 and Ravi Shridhar, MD-PhD2 1 Epidemiology Division and 2 Gershenson Radiation Oncology Center Barbara Ann Karmanos Cancer Institute Detroit Medical Center Wayne State University Detroit, MI
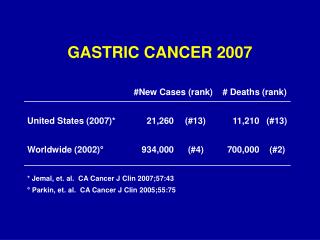
Gastric Cancer Epidemiology • 870,000 new cases gastric cancer/year worldwide. • 650,000 deaths/year worldwide, (75%). • 22,000 new cases/year in US in 2006. • 11,430 deaths/year, (52%) Lower ratio in US. • Gastric Cancer is 14th in incidence in US. • Worldwide top 3 cancers are lung, breast, colon. • Top 3 deaths from cancer are lung, gastric, and liver.
Gastric Cancer Epidemiology • Location of gastric tumors are most common in the antrum. • Antrum or distal stomach 40% • Fundus, cardia, GEJ 35% • Body 25%
Gastric Cancer Epidemiology • Worldwide decline over past few decades • 1930-1980 • Decrease from 38 to 10/100,000 men, • Decrease from 30 to 5/100,000 women. • Identification and treatment of Heliobacter pylori. • Dietary factors • Fresh fruits and vegetables (antioxidants) • Introduction of refrigeration • Less salt based preservation (includes nitrates) • Less bacterial and fungal contamination
Patterns of Spread • Direct • Omenta, pancreas, diaphragm, colon, duodenum, jejunum, vessels, adrenals, kidney • Lymphatic • Paracardial, lesser and greater curvature, pyloric, celiac, SMA, hepatic, splenic, paraaortic • Hematogenous • Via portal system • Peritoneal • Often diffuse process
Staging – Japanese • N1 – stations 1-6 • Paracardial, greater and lesser curvature, pyloric • N2 – stations 7-11 • Left gastric, common hepatic, splenic art and hilum, celiac • N3-4 – stations 12-16 • Hepatic, retropancreatic, mesenteric root, middle colic, paraaortic
T1: invasion of the lamina propria T2a: invasion of the muscularis T2b: invasion of the subserosa T3: penetration of the serosa (visceral peritoneum) T4: invasion of adjacent structures N1: 1-6 lymph nodes N2: 7-15 lymph nodes N3: >15 lymph nodes Gastric Cancer AJCC Staging
Gastric Cancer AJCC Staging } 1 } 2 } 3 } 4 } 5 • Stage IA T1 N0 • Stage IB T1 N1 • T2 N0 • Stage II T1 N2 • T2 N1 • T3 N0 • Stage IIIA T2 N2 • T3 N1 • T4 N0 • Stage IIIB T3 N2 • Stage IV T4 N1-3 • T1-3 N3 • M1
Lymph Node Ratio • Lymph Node ratio = (LNR = LN pos /LN exam) • - LN pos = number lymph nodes positive • - LN exam = number nodes examined • Nodal ratio has become an important prognostic tool • Studies showing importance of nodal ratio in rectal, pancreatic, and gastric cancer • Nodal ratio in breast cancer predicts for survival, recurrence and who benefits from Radiation Therapy. • No large US lymph node ratio gastric studies.
Aims • The first aim of this study was to compare three measures of lymph node involvement as a predictor of gastric cancer survival • Number of Total nodes examined, • Number of Total metastatic nodes, and • Lymph Node Ratio (LNR) (metastatic nodes)/(nodes examined). • The second aim was to examine the effect of removing 15 or more lymph nodes on survival outcomes for N0-N2 and 30 or more for N3
Methods • Data contained 13,745 cases of gastric cancer taken from the Surveillance, Epidemiology and End Results (SEER) 1990-2003 public access data tapes. • Data were grouped by N0, N1, N2, and N3 stages (AJCC) as well as Lymph Nodes Examined, Lymph Nodes Positive and Lymph Node Ratio (LNR); (LNR = LN pos /LN exam). • Survival analysis was conducted with SAS ver 9.1 utilizing proc lifetest for the Kaplan-Meier analysis and proc phreg for Cox proportional hazard analysis.
Results r=0.8 P<0.0001
Results r=0
Results AC - Adenocarcinoma
Conclusion • LNR is a simple, significant predictor for survival. • Removing >15 lymph nodes provided a survival benefit across stages N0, N1 and N2. • LNR as a predictor of survival was nearly identical whether <15 or >15 lymph nodes were removed. • LNR should be considered in the staging system.