Download

1 / 38
380 likes | 535 Views
THE EVOLUTION OF SENIORS’ FALLS PREVENTION IN BRITISH COLUMBIA. Dr. Vicky Scott, Lillian Baaske, Dorry Smith, Tessa Graham, Dr. Elaine Gallagher, Dr. Ian Pike, Matt Herman & Mike Vanderbeck. B.C. Seniors. Those 65+ account for 13.7% of the B.C. population

E N D
THE EVOLUTION OF SENIORS’ FALLS PREVENTION IN BRITISH COLUMBIA Dr. Vicky Scott, Lillian Baaske, Dorry Smith, Tessa Graham, Dr. Elaine Gallagher, Dr. Ian Pike, Matt Herman & Mike Vanderbeck
B.C. Seniors • Those 65+ account for 13.7% of the B.C. population • 1995 to 2004 population 65+ rose from 475,300 to 574,400 (21% increase) • 2004 to 2010, number of seniors is expected to grow by another 17% to 672,000 • Between 2001 to 2021 the average age in B.C. will increase from 38.2 to 42.6 years
Outline • Laying the Groundwork • Policy Considerations • Environmental Scan in B.C. • Translation of Research to Practice • The Interior Health Authority Experience
Laying the Groundwork for B.C.’s Success • 15 years of sustained collaboration • Champions positioned to support and influence • Recognition of opportunities and timing • Shared vision and commitment • Leadership • Strategic investment of limited resources • Strategic multi-sectoral partnerships • Involve the right people in decisions, including those affected by the problem • Respect for roles and responsibilities
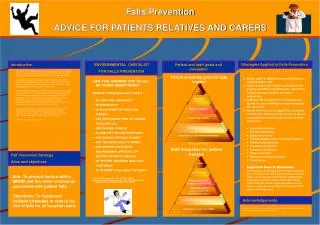
Essential Questions for Falls Prevention Planning • What is the nature and magnitude of the problem in your region? • What policies do you need to support prevention? • Who should be involved in prevention? • Who is at risk for falls and injuries? • What are the best prevention strategies? • How will you know if the strategies work? • How will prevention efforts be sustained?
Falls & Injury Prevention Planning Scott et al., 2005. Evolution of Seniors’ Falls Prevention in British Columbia What is the nature and magnitude of the falls in your region? Who is at risk for falls and injuries? What are the best practices and prevention strategies? RESEARCH Are you using the best data sources to highlight the problem? Do you know how the problem has changed over time and what is expected in the future? Do you know the economic burden of falls for your region and how this compares to other health issues and other regions? What are the risk factors for falling and sustaining a fall-related injury? Who is at greatest risk? How does risk vary across sub-populations of men and women, active seniors vs. frail seniors in the community, seniors in acute care or residential settings? How do we know what works best to reduce risk and minimize outcomes? How do we know what will work in practice? What policies are needed for strategies to be effective? Can you translate the evidence into a business case for resources to support cost-effective prevention? What are the most reliable sources of evidence? How will you engage policy makers, health care managers and agencies to support your research and translation efforts? What policies do you need to support evidence-based prevention? POLICY Who in your region is conducting research on falls prevention? Can you access those who are able to identify reliable sources of research and translate findings into effective practice? Can research be used to create a climate for this issue? What evidence is needed before this issue will gain the support of policy-makers and those that will resource prevention efforts? What evidence do you need to affect decision-making, program planning, evaluation and resource allocation? Who has the greatest potential for effecting change in policy and practice? Who will fund research efforts? What policies, regulations or guidelines do you need to support falls prevention? How will you know if the strategies work? How will prevention efforts be sustained? PRACTICE What will be evaluated? What process and outcome measures will you use? How will you know if your strategies are cost-effective? How will you know if there are gaps in your efforts? How will you share this information and for what purpose? How will you use the evaluation outcomes to improve your prevention plan? What research and policy support do you need to maintain effective prevention efforts? How will you resource the strategies? What time commitments are required? Will you engage those at risk, volunteers, staff and managers? How will you contact your target audience? Who has the greatest potential for planning, implementing and evaluating prevention activities?
Policy Considerations • Action on falls did not happen overnight • Important ingredients: policy decisions, champions, evidence, opportunities and timing • Collaborative jurisdictional action on aging: the context
Policy Considerations • Key policy and documents commissioned/released by F/P/T Ministers • Evidence led to action and engagement of experts and those affected by the problem • Commitment to injury prevention and falls was built over time • Nationally unique partnership between Health Canada and Veterans Affairs launched in 2001
Policy Considerations • Continued federal/provincial/regional collaboration following the HC/VAC program • Critical mass of individuals involved at different levels in the issue developed: state of readiness to act • Environment created to support further collaboration • Development and release of the Environmental Scan: Seniors and Veterans Falls Prevention Initiatives in B.C. 2005 • Establishment and support of BC Falls Prevention Coalition 2005
Ottawa Charter (1986) National Framework on Aging (1998) BC Office for Injury Prevention (OIP) – focus 0-24 years Deputy PHO created BCIRPU – focus on all ages (1997) BC Summit on Falls Prevention (1998) F/P/T Ministers of Health and Safety and Security Working Group (SSWG) (1999) – Seniors’ injury seen as priority F/P/T Advisory Committee on Population Health - Sub-committee of Public Health – Falls Among Elderly seen as priority Overview of Activities
Activities Continued • OIP and B.C. Office for Seniors jointly created Falls Prevention Specialist position (2001) • Veterans Affairs and Health Canada Falls Initiative (2001-2004) • Special PHO report on Falls and Injuries among the Elderly (2004) • Partnership with Knowledge Network for social marketing of falls prevention (2004) • BC Falls Prevention Coalition (2005)
B.C. Research History • Scope of the problem • Risk factor evidence • Prevention evidence • Capacity building • Sustainability • Dissemination
Scope of the Problem • First profiled as a serious issue in B.C. in 1989 at an Inter-ministerial Committee on Aging • MOH led a provincial meeting on fall-related hospitalizations (Dr. Bob Fisk, 1990) • 1st RCT on falls in B.C. “Head Over Heels” (Gallagher & Brunt, 1991) • Health Canada funded the “STEPS” project on falls in public places (Gallagher & Scott, 1994) • Mortality and Morbidity of Falls in B.C. (Scott & Gallagher, 1997 )
Risk Factors & Prevention • U.Vic: Risk factors for falls and injuries among frail community seniors (Scott & Gallagher, 2000) • Population Health/BCIRPU: “Stepping In” Fall Prevention in LTC (Scott et al., 2003) • BCIRPU: EDISS Reports on Fall Injury in Emergency Dept. (2004); “SAIL” Pilot and RCT (Scott et al., 2004/2005) • UBC: Risk reduction for women with osteoporosis (Lui-Ambrose & Kahn, 2003); Strength & Balance in Reducing Falls (Donaldson & Kahn, 2005); Fall Risk for Women with Visual Impairment (Szabo & Kahn, 2006); ED Fall Outcomes (Salter, 2004) • SFU: Biomechanics of Falls & Hip Fractures (Robinovitch, 2005); Floor Stiffness & Risk of Hip Fracture (Laing, 2003-) • Other: Paramedics for Early Intervention of Falls (Robinson, 2004); OT Falls Assessment (Dixon, 2004); Centre for Hip Health (Oxland, 2006)
Capacity Building, Sustainability & Dissemination • F/P/T: Systematic Review of Best Practice in Falls Prevention (2000) • F/P/T: National Inventory of Falls Prevention (2000) • BCIRPU: Economic Burden of Unintentional Injury in B.C. (Smartrisk, 2001); Unintentional Fall-related Injury and Deaths: Trends, Patterns & Projections (BCIRPU, 2002) • MOH/BCIRPU: Prevention of Falls & Injury Among the Ederly: PHO Report • PHAC/MOH: Environmental Scan: Seniors & Veterans Falls Prevention Initiatives in B.C.
Fall-related Hospital Rates per 1,000 by Provinces and Territories, 1998/99 – 2002/03, Ages 65+
Environmental Scan Environmental Scan of Seniors and Veterans Falls Prevention Initiatives • Dr. Vicky Scott, Senior Advisor on Falls Prevention, BCIRPU • Dr. Elaine Gallagher, Professor, UVic School of Nursing • Dr. Mariana Brussoni, Associate Director, BCIRPU • Kristine Votova, Doctoral Student, University of Victoria • Dorry Smith, Researcher, BCIRPU
Purpose and Background • Why falls? • 85% of all injuries to the elderly • $180 million in direct health costs (BC,1998) • Why a falls’ inventory? • Reflect changes since the previous scan (Scott, Dukeshire, Gallagher, & Scanlan, 2001) • Aid practitioners/researchers to better understand critical factors • End result: prevent falls, promote networking and contribute to a collective effort currently underway in the province to reduce falls and injuries among older persons
Methods of Data Collection • Epidemiological data • Vital Statistics (mortality) • Ministry of Health (hospital separation) • Inventory data • Province-wide survey of seniors falls prevention initiatives • Critical factors of success • In-depth interviews with successful programs
Results • 116 completed inventories submitted • Nine-fold increase in reported initiatives • Initiatives categorized: • Policy • Research • Practice
Results • Community/Pre-Frail and Well-Elderly (32%) • LTC/Frail and Cognitively Impaired Elderly (30%) • Acute Care/Geriatric Rehab Services (5%) • Cross-Site (11%) • Research (11%) • Policy (8%) • Private Providers (3%)
Information Provided in the Scan • Initiatives’ descriptive information • Key findings of critical factors of success • Recommendations to healthcare settings and providers • Indexes of tables
Evidence-based Applicable Affordable Effective Sustainable Translating Research to Practice
Evidence to Practice Example The Interior Health Authority experience • 1995: Researchers bring the issue of falls to the region • 2000: North Okanagan Health Region (NOHR) planners were alarmed at the high rate of falls for their Health Area
Evidence to Action • Partnerships formed • Communities buy-in • Three year funding received from HCVAC
Climate for Change • Four health areas merge in 2000 creating a climate change • New health region holds Population Health Conference in 2002 and Falls Program is showcased • Aging Population = Higher Falls Numbers
Pop Health Jump Starts Falls Focus • Champions were identified • Project funds were strategically dispersed • Strategic Plan was drafted • Falls Prevention Manager appointed by Population Health to provide leadership and support of regional efforts
Building Capacity • Created inventory with BCIRPU • Hired BCIRPU to produce a comprehensive falls report • Identified and supported falls pilots in each sector and health area based on sound research/best practices • Working with Municipal Councils, community groups and seniors to develop partnership to address local fall issues
Action to Practice Internal: • Residential Falls Program • Acute Care Project • Community Health Care Workers Project External: • Safe Communities falls prevention program
Challenges • Constant change • Compliance (Forms) • Reliable “real time” internal data • Developing universal reporting systems • Sustaining the programs beyond the project phase
Next Steps in Interior Health • Mandatory Performance Management indicators • Across sector falls reports • Hand over clinical piece to Performance Management • Will expand focus to include assisted living and well seniors in the community
What we have learned in B.C. • It takes time • Need the evidence • Need the right partners • Need to integrate prevention into policy and practice • Need to evaluate and disseminate • Need to build sustainability in from the start • Need to celebrate your successes
Next Steps for B.C. • CFPC – national standardized training – B.C. climate created opportunity to do this • Accountability by HAs and Professionals • Regional performance indicators • Setting-specific practice indicators • BCFPC • Monitoring and supporting • Priority setting • Disseminating
Questions? Thank You! Merci!