Download
1 / 40
450 likes | 578 Views
Diseases of Stomach. Aim: to understand the pathogenesis of gastritis, peptic ulcer disease and cancer of stomach. Stomach. Stomach. Histology Cell types – mucous cells parietal cells chief cells endocrine cells.

E N D
Diseases of Stomach Aim: to understand the pathogenesis of gastritis, peptic ulcer disease and cancer of stomach.
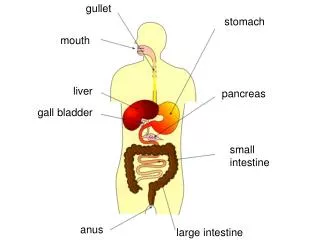
Stomach • Histology Cell types – mucous cells parietal cells chief cells endocrine cells.
Gastric mucosal protection: Intraluminal concentration of H+ is 3 million times greater than blood and tissue. “Mucosal barrier” 1] Mucous secretion. 2] Bicarbonate secretion. 3] Epithelial barrier (rapid regeneration). 4] Mucosal blood flow (to sweep away hydrogen ions). 5] Prostaglandin protection (help maintain blood flow).
Diseases of Stomach • Clinical manifestation of gastric disease: - pain and dysphagia - loss of appetite - bleeding (hematemesis or melena ) - gastric mass - gastric outlet obstruction
Diseases of Stomach • Gastritis • ACUTE • CHRONIC • Gastric ulcer • ACUTE • CHRONIC
Diseases of Stomach • Gastritis - Inflammation of gastric mucosa. - Could be acute or chronic.
Chronic (non-erosive) gastritis • Chronic gastritis is defined as the presence of chronic inflammatory changes in the mucosa leading eventually to mucosal atrophy and epithelial metaplasia. • It is notable for distinct causal subgroups and for patterns of histologic alterations that vary in different parts of the world.
Chronic (non-erosive) gastritis Types: • Type A: chronic atrophic gastritis (Autoimmune gastritis) • Type B: Helicobacter pylori associated gastritis
Type A chronic atrophic gastritis (Autoimmune gastritis) • Account for less than 10% of chronic gastritis. • Autoantibodies to gastric glands parietal cells and intrinsic factor • Lead to gland destruction with atrophy, loss of acid production ( achlorhydria) and inflammation. • Hypergastrinemia occurs secondary to hyperplasia of the G (gastrin) producing cells in the antrum. • Patient develops pernicious anaemia. • Associated with other autoimmune disease (e.g., Hashimoto thyroiditis, Addison disease) • There is increased incidence of adenocarcinoma (10%) and cacinoid tumor
Helicobacter pylori associated gastritis • Most important etiologic factor found in 90% of patient with chronic gastritis. • Infected persons: increased risk for peptic ulcer and gastric carcinoma and lymphoma. • Helicobacter pylori, nonsporing, curvilinear gram negative rod, motile organisms. It elaborate urease and attach itself to gastric epithelial cells. • Preduce cytotoxin and endotoxin. • Symptoms improved after antimicrobial agents.
Schematic presentation of the presumed action ofHelicobacter pylori in the development of chronic gastritis. - H. pylori produce urease and toxins, including lipopolysaccharide, cagA, and vacA. -These, in concert with host-derived gastric acidity and peptic enzymes, produce a chronic state of gastric mucosal injury leading to chronic gastritis.- Note that H.pylori do not colonize regions of intestinal metaplasia.
After initial exposure to H. pylori, gastritis may develop in two patterns: • (1) an antral-type with high acid production and higher risk for the development of duodenal ulcer • (2) a pangastritis with multifocal mucosal atrophy, with low acid secretion and increased risk for adenocarcinoma
Chronic (non-erosive) gastritis • Histologic features • Both types (A & B) - chronic inflammation in lamina propria with varying degrees of atrophy; metaplasia and dysplasia may occur; mostly in type A associated with pernicious anemia • Type A - loss of parietal cells • Increased risk of gastric carcinoma (Types A & B), especially when associated with pernicious anemia
Chronic gastritis showing partial replacement of the gastric mucosal epithelium by intestinal metaplasia (upper left) and with inflammation of the lamina propria involving (right) lymphocytes and plasma cells.
Morphology of Chronic Gastritis • In helicobacter pylori, inflammation affect antral mucosa mainly, while autoimmune gastritis, there is diffuse mucosal damage mainly of body-fundic mucosa. • Active inflammation-neutrophil within glands. • Regeneration changes. • Intestinal metaplasia. • Atrophy • Hyperplasia of gastrin-preducing cells. • Dysplasia.
Chronic Gastritis Clinical features: • Usually few symptoms of upper abdominal discomfort and vomiting. • Achlorhydria, hypergastrinaemia and anemia in autoimmune gastritis. • The relationship of chronic gastritis with the development of peptic ulcer, gastric carcinoma and lymphoma is present.
Persons with chronic gastritis and H. pylori usually improve symptomatically when treated with antibiotics and proton pump inhibitors.
Acute gastritis • Usually of a transient nature. • May be accompanied by hemorrhage or sloughing of the superficial mucosa. • Frequently associated with heavy use of: • aspirin and NSAID • alcohol, smoking • Chemotherapy • Uremia • systemic infection • severe stress (trauma, burns) • ischemia • suicidal attempts • gastric irradation.
Acute gastritis • Mild: edema and vascular coungestion, scattered neutrophil in mucosa. • Severe: erosion of mucosa, hemorrhage, acute inflammatory infiltrate (acute erosive gastritis). • May be asymptomatic or present with gastric pain, vomiting, hematemesis, melena (may lead to fatal blood loss).
Diseases of Stomach • Gastritis • ACUTE • CHRONIC • Gastric ulcer • ACUTE • CHRONIC
Peptic Ulcer Disease • Ulcer: a breach in the mucosa of the alimentary tract extending through muscularis mucosa into submucosa or deeper. • Peptic ulcers are chronic, most often solitary occuring in any part of GIT exposed to the action of acid gastric juice. • Sites: Duodenum (first part), lower esophagus, stomach ulcer, Meckel’s diverticulum, jejunum, ileum and colon (Zollinger-Ellison syndrome)
Peptic Ulcer Disease Epidemiology: In USA, 350,000 new cases – 3,000 die yearly as result of peptic ulcer. • Peptic ulcer are remitting, relapsing lesion. • Diagnoses in middle-aged to older adults. • M:F = 3:1. • Decrease in prevalence of duodenal ulcers. • Genetic influences –little or no role. • Duodenal ulcer – more in alcoholic cirrhosis, COPD, chronic renal failure and hyperparathyroidism (hypercalcaemia increase gastrin production).
Peptic Ulcer DiseasePathogenesis: • Two conditions are key for the development of peptic ulcers: • (1) H. pylori infection, which has a strong causal relationship with peptic ulcer development • (2) mucosal exposure to gastric acid and pepsin.
Peptic Ulcer Disease Pathogenesis: • Other causes: • Abnormal gastric mobility. • Others: • NSAID • Corticosteroid • Aspirin • Stress • Cigarette smoking • Zollinger Ellison syndrome • Alcoholic cirrhosis
Peptic Ulcer Disease • Helicobacter pylori is present in 70% to 90% in pt. with duodenal ulcers and 70% of gastric ulcer • Only 10% to 20% of infected people develop peptic ulcer • Mechanisms include • H. pylori induces an intense inflammatory reaction (IL-1, IL-6, TNF and IL-8) • Several bacterial products (urease, phospholipase, VacA and CagA) • Enhance gastric acid secretion and impair bicarbonate production • H. pylori is immunogenic
Pathogenesis of Ulcers Therapy is directed at enhancing host defense or eliminating aggressive factors; i.e., H. pylori. Aggressive Factors Acid, pepsin Bile salts Drugs (NSAIDs) H. pylori Defensive Factors Mucus, bicarbonate layer Blood flow, cell renewal Prostaglandins Phospholipid Free radical scavengers
Peptic Ulcer Diseasepathology • 98% located in first portion of duodenum or stomach, ratio = 4:1 • Solitary – 1 to 5 cm. • Margin – flush, edematous. • Floor –smooth. • Base – thick and firm (fibrosis). • Surrounding mucosa – normal to chronic gastritis. • Deep ulceration, perforation.
Peptic Ulcer Radiating mucosal folds
Peptic Ulcer Disease Clincal features • Epigastric pain, worse at night, relieved by food and anti-acid • Nausea, vomiting, belching and weight loss • First presentation with complications • Chronic recurrent
Peptic Ulcer Disease Complications • Bleeding • Perforation • Pyloric obstruction • Malignant transformation, v. rare in gastric peptic ulcer
Acute Gastric Ulceration • May appear after stress (Stress Ulcer) • Multiple lesions in stomach and duodenum • Most commonly encountered in: - sever trauma - extensive burns ( Curling Ulcer) -Trauma or surgical injury to CNS (Cushing Ulcer) - Chronic exposure to gastric irritant. • The outcome depends on the ability to control underlying conditions.
SUMMARYInflammatory Diseases of the Stomach • Chronic gastritis: • major cause is infection by Helicobacter pylori, less commonly autoimmune in origin • characterized by mononuclear cell infiltration in the lamina propria with intestinal metaplasia and frequently, proliferation of lymphoid tissue • may be the precursor of peptic ulcer and carcinoma. • Acute gastritis: acute mucosal inflammation, usually transient, associated with use of NSAIDs, alcohol, heavy smoking, and various systemic abnormalties
SUMMARYInflammatory Diseases of the Stomach • Peptic ulcer: breach in the epithelium • caused most commonly by H. pylori infection and mucosal exposure to gastric acid and enzymes (pepsin), or less frequently by use of NSAIDs • sharply demarcated mucosal defects with underlying necrosis, acute inflammation, granulation tissue, and scarring • manifested by bleeding and, less commonly, rupture. • Stress ulcers (acute gastric ulcers): • associated with severe trauma, burns, CNS trauma or hemorrhage; usually small, multiple, hemorrhagic ulcers that are often shallow