Download
1 / 46
460 likes | 485 Views
This study examines the impact of sodium restriction on renoprotective therapy outcomes in chronic kidney disease (CKD) patients, highlighting the importance of low-sodium diet in conjunction with ACE inhibitors. The research emphasizes the significance of controlling salt intake for better blood pressure and proteinuria management in CKD patients. Results show that sodium restriction potentiates the effects of ACE inhibitors, with the lowest blood pressure and proteinuria observed in patients on a combination of low-sodium diet and diuretics. The study underscores the role of dietary sodium restriction in improving renal and cardiovascular outcomes in CKD patients, independent of blood pressure control. Excessive salt intake is associated with poorer renal outcomes despite well-managed blood pressure levels. The protective effect of sodium restriction extends beyond blood pressure control and is particularly beneficial in diabetic patients.

E N D
Beneficial effects of sodium restriction on outcome of renoprotective therapy in CKD Gerjan Navis UMCG Groningen The Netherlands
Saltintake around the world Recommended
Sodium restriction and ACEi in essential hypertension • RAAS-blockade potentiates effect of low Na+ diet • RAAS-blockade makes blood pressure sodium sensitive in all patients! Navis, J Cardiovasc Pharm 1987: 9: 743-8
Low sodiumdietincreases top of dose-responseforACEionbloodpressure and proteinuria Experimental nephrotic syndrome Wapstra, Cli Sci 1996: 90: 393-401
Controlof sodiumexcessimprovestherapy response in CKD MAP, mmHG Uprot, g/d ACEI ACEI Buter, NDT 1998: 13: 1682 Heeg, Kidney Int 1989; 36,272
Effect of sodium status ontherapyresponse to CCBin diabeticnephropathy Diltiazem Nifedipine Ualb mg/d MAP, mmHG Sodium-dependency of Rx-response may depend on specific drug characteristics Proteinuria can respond to low sodium in the absence of a BP response Bakris, Ann Int Med 1996: 125: 201-204
Excess sodium blunts the effects of RAAS-blockade, even during diuretic therapy • Low sodium diet reduces blood pressure and proteinuria • Low sodium diet potentiates effect AT1RA on blood pressure and proteinuria, plm equivalent to diuretic • Lowest blood pressure and proteinuria during combination low sodium/diuretic • NB: target LS: 50 mmol/d • Obtained: 90-100 mmol/d ! Vogt et al: J Am Soc Nephrol 2008;19: 999-1007.
Sodium restriction more effectively potentiates ACEi than dual blockade Plm 180 mmol/d plm 100 mmol/d Slagman et al, BMJ 2011, 343:d4366
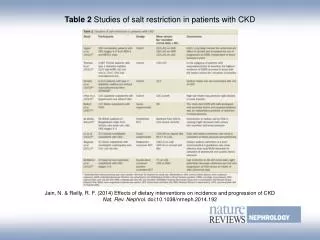
REIN trial: outcome by mean salt excretion/2 yrs CKD patients, overt proteinuria ACEi vs conventional AHT Titration of BP to < 140/90 Salt intake by tertiles of urinary sodium: LSD: plm 5-7 g/d MSD: plm 10-12 g/d HSD: plm 15 g/d Vegter, JASN 2012: 23: 165-73
REIN trial: need for diuretics • BP control was independent of sodium intake • However, MSD and HSD required more diuretics than LSD LSD MSD HSD LSD MSD HSD Vegter, JASN 2012: 23: 165-73
Results - proteinuria At inclusion (before ACEi): LSD: 2.0 g/g MSD: 2.1 g/g (P=0.014) HSD: 2.6 g/g (P=0.011) During treatment: Worse antiproteinuric efficacy, Proportional to salt intake
REIN TRIAL: hard renal end points by salt intake Excessive salt intake is associated with worse renal outcome, DESPITE well-controlled blood pressure ! Vegter, JASN 2012: 23: 165-73
Dietary sodium restriction provides renoprotection beyond blood pressure control !
RENAAL-IDNT: Effect of sodium status on outcome Lambers Heerspink Kidney Int 2012: 82: 330-337.
RENAAL-IDNT: salt excess annihilates renal and CV protection by ARB No. of events / patients Hazard Ratio (95% CI) Favours Favours p for ARB Non-RAASi ARB Non-RAASi trend Renal Outcome Na:Cr <121 mmol/g 40/173 75/219 0.57 ( 0.39 - 0.84 ) 121<Na:Cr <153 mmol/g 54/175 72/218 1.00 ( 0.70 - 1.42 ) <0.001 Na:Cr ≥ 153 mmol/g 56/151 75/241 1.37 ( 0.96 - 1.96 ) Overall 150/499 222/678 0.92 ( 0.75 - 1.14 ) Cardiovascular Outcome Na:Cr <121 mmol/g 45/173 64/219 0.63 ( 0.43 - 0.92 ) 121<Na:Cr <153 mmol/g 62/175 62/218 1.02 ( 0.73 - 1.43 ) 0.021 Na:Cr ≥ 153 mmol/g 59/151 72/241 1.25 ( 0.89 - 1.75 ) Overall 166/499 198/678 0.93 ( 0.75 - 1.15 ) 2.0 0.5 1.0 1.5 Hazard ratio (95% CI) Lambers Heerspink Kidney Int 2012: 82: 330-337.
RENAAL-IDNT: salt excess annihilates renal and CV protection by ARB No. of events / patients Hazard Ratio (95% CI) Favours Favours p for ARB Non-RAASi ARB Non-RAASi trend Renal Outcome Na:Cr <121 mmol/g 40/173 75/219 0.57 ( 0.39 - 0.84 ) 121<Na:Cr <153 mmol/g 54/175 72/218 1.00 ( 0.70 - 1.42 ) <0.001 Na:Cr ≥ 153 mmol/g 56/151 75/241 1.37 ( 0.96 - 1.96 ) Overall 150/499 222/678 0.92 ( 0.75 - 1.14 ) UNaV 152/d 179/d 209/d Cardiovascular Outcome Na:Cr <121 mmol/g 45/173 64/219 0.63 ( 0.43 - 0.92 ) 121<Na:Cr <153 mmol/g 62/175 62/218 1.02 ( 0.73 - 1.43 ) 0.021 Na:Cr ≥ 153 mmol/g 59/151 72/241 1.25 ( 0.89 - 1.75 ) Overall 166/499 198/678 0.93 ( 0.75 - 1.15 ) 2.0 0.5 1.0 1.5 Hazard ratio (95% CI) Lambers Heerspink Kidney Int 2012: 82: 330-337.
Protective effect sodium restriction in CKD/DMII predominantly related to lower albuminuria Lambers Heerspink , 2012, submitted
Effects of sodium intake on outcome in CKD during RAASi:similar for DM and non-DM !! Lambers Heerspink, NDT 2012, 27: 3435-42
Resume so far • Modest reduction of dietary salt, towards targets recommended for the general population is associated with substantial renal and cardiovascular benefits in renal patients • Modest dietary sodium restriction provides cardio-renal renoprotection beyond blood pressure control ! • Use of diuretics does NOT overcome effect of salt excess on hard end points • The beneficial effect of avoiding sodium excess is also present in diabetic patients
de Volkskrant 22 september 2012 Voorgeschreven maar te licht bevonden “Grote kans dat er in uw medicijnkastje pillen staan die u dagelijks slikt, misschien al jaren, en die door de verzekeraar worden betaald terwijl ze helemaal niet werken. Bloeddrukverlagers: 4 miljoen gebruikers. Kosten 390 miljoen euro”. “Onderzoek heeft vastgesteld dat een bepaald medicijn, zogeheten ACE-remmers, bij een kwart van de hartpatiënten niet werkt. Het is onbekend waarom. Bijna een miljoen Nederlanders gebruiken zo'n ACE-remmer”.
Mechanisms 1: the volume component Effect of low sodium and/or diuretic is predicted by NT-proBNP Slagman et al NDT 2011.
Alleged mechanisms of interaction sodium status and response to RAAS-blockade • Sodium loading stimulates vascular and renal tissue ACE • Sodium loading has pro-inflammatory effects • Other??
Mechanisms: High salt blocks tissue effects of ACEi ACEi, LOW SODIUM ACEi, HIGH SODIUM Kocks MJA, J Cardiovasc Pharmacol 2003: 42:601-05
Effect of sodium status on urinary CTGF in CKD Slagman CJASN 2011
VEGF-c responds to high salt in CKD and controls human evidence for non-volume Na-induced pathways Healthy subjects CKD Slagman et al, NDT 2012
Issues to consider • How low should we go? Can we go too low? • Short term renal function decline : a reason for concern? • Recent studies claiming that high salt is beneficial • Feasibility • How do I titrate volume status?
Low sodiumdietincreases top of dose-responseforeffects of ACEionbloodpressure and proteinuria Experimental nephrotic syndrome: lower BP and UP did not translate into better protection against FGS Wapstra, Cli Sci 1996: 90: 393-401
Dissociation of BP & proteinuria from interstitial fibrosis during ACEi-low salt: adriamycin nephrosis SBP: 111+19 mmHg UP 350 + 239 mg/24h Pcr 4.6 + 1.3 mg/L FGS: moderate/severe IF: moderate ACEi SBP: 102+19 mmHg UP 48 + 17 mg/24h Pcr 4.6 + 1.4 mg/L FGS: mild/absent IF: severe !!!!! ACEi: low salt Non-invasive markers for fibrosis needed!!! Hamming, J Pathol 2006: 209: 129-39
Is there a J-curve for sodium intake ?All-cause mortality by 24h UNaV T2DM T1DM 24-h UNaV Thomas, Diabetes Care 2011, 34: 861-6 Lambers Heerspink, 2012
Saltintake from UNaV in CKD cohorts MASTERPLAN REIN VITAL STENO studies De Nicola et al Recommended
Issues to consider • Short term renalfunctiondecline : a reasonfor concern? • Recent studies
Reversible renal function declineinteraction sodium restriction with single/dual RAAS-blockade Reduction in renal function by sodium restriction is prominent during dual blockade, with only subtle added therapeutic effect Slagman et al, BMJ 2011, 343:d4366
Issues to consider • How low should we go? Can we go toolow? • Short term renalfunctiondecline : a reasonfor concern? • Recent studies claimingthat high salt is beneficial • Confoundingby “indication” ? • Do not consider therapy effects ! • Should NOT simlybeextrapolated to the clinical setting in renalpatients
Issues to consider • Feasibility • Has been proven in TOPH in primary care settings • Has been proven in outpatient nephrology settings • 24h urine provides unbiased measure of sodium intake: this helps to improve dietary habits (and overcome poor food labelling) • Should never be an excuse ! • Novel tools: e-health & self management for sustainable lifestyle modification (ZON-MW doelmatigheid 2013)
Dietary Na+ restriction reduces CV events and mortality on long term follow up (TOHP I and II) • Prehypertensive subjects • Dietary counseling n=327/1191, control 417/1191 • Baseline sodium excreton 150/182 mmol/d • Reduction 50-40 mmol/d TOHP I Cook, BMJ, april 20, 2007
Global lifestyle improvementthe Finnish Experience Salt BMI Smoking Karpaten & Mervalaa, 2006: 49: 59-75
Global lifestyle improvementthe Finnish Experience Blood pressure Life expectancy CHD mortality HEALTH BENEFITS Karpaten & Mervalaa, 2006: 49: 59-75
Call for action ! • Better salt awareness is a must ! • Modest reduction dietary salt is already associated with substantial benefits in renal patients, including diabetics • 24-h urine is an extremely valuable source of dietary information ! • Counsel & support individual patients • Target government and industry • Hard end point trials are within reach !!!!
Acknowledgements: Liffert Vogt Femke Waanders Maartje Slagman Arjan Kwakernaak Stefan Vegter Hiddo Lambers Heerspink Dick de Zeeuw Piero Ruggenenti Giuseppe Remuzzi Anna Lisa Perna Marina Noris HOLLAND NEPHROLOGY STUDY GROUP Goos Laverman Marc Hemmelder Arend Jan Woittiez Wilbert Janssen