Download
1 / 36

E N D
To code, or not to code: that is the question: Whether 'tis nobler in the mind to suffer (786.5) The calls and emails of outrageous fortune,Or to take arms against a sea of uncoded T’cons,And by opposing end them? To be denied leave, and sleep (307.41)No more; and by taking leave we temporarily endThe heart-ache (419.9) and the thousand emailsThat my in-box is heir to, 'tis a consumption (011.9)Devoutly to be wish'd against. Jim Cox, in his year of discontent 2005
Coding Overview and the Commander’s Statement Ms Sharon Taylor June 2006 DQMC
Goal • Quality data on which to base sound decisions
Data Goal Corollary • You give me bad data, I’ll make bad decisions
Suggested Coding “Solution” • Have each new provider, prior to receiving privileges to practice at your MTF, spend 4 hours with a good coding trainer • Option to “test out” of the class by passing test composed of examples of quality documentation which the provider will enter the correct diagnoses/external causes of injury, evaluation and management code(s) with modifiers, procedure code(s) and any other applicable HCPCS code(s)
One-on-one Training Overview • Each training is specific to the specialty involved (e.g., training is different for obstetrics, orthopedics and occupational therapy) • 1 hour documentation/diagnoses • 1 hour evaluation and management/modifiers • 1 hour procedures/supplies/training • 1 hour practice
Training Goals • Learn basics of good documentation • Learn basics of ICD/E&M/CPT/HCPCS coding • Learn when to ask for coding assistance • Become comfortable asking coder questions (it also gets the coder comfortable working with the provider)
Measure Success of Training • Random audit of provider’s first week of documentation/coding and provide immediate feedback • Random audit of provider’s first month and provide immediate feedback • Continue to audit/provide one-on-one feedback until documentation and coding are consistently at acceptable level
Professional Staff • Arrange to have coder auditor have maximum of 5 minutes at professional staff to review issues common to the facility • Arrange to have coders permitted to attend professional staff as • This will permit a non-threatening environment for providers and coders to interact • Coders need continuing education too
Objectives • Understand Data Application • Understand What the Data Are and Are Not Indicating • Understand “Random” When Applied to Audits
Running a Business • Would you like to know • Your customers • How much it costs to make your product • For how much you can sell your product
Running a Business • Would you like to know • Your customers • ICD-9-CM diagnosis data (6c) • Demographic data • Patient categories (PATCATs) • How much it costs to make your product • Medical Expense Performance and Reporting System (MEPRS) • For how much you can sell your product • Relative Value Units (RVUs) and Relative Weighted Products (RWPs) (6b and 6e)
Data Quality = $$$ • Patient Registration • PATCATS - $$$ - • $180.8M last year (get your Coast Guard, VA, DoD civilians, and civilian emergencies correct…) • Identifying injuries (Medical Affirmative Claims) - $$$ • $16.5M last year – demonstrates how poorly we identify these cases • Other Health Insurance (DD 2569) - $$$ • $106.3M last year • Documentation - $$$ • Must have document filed in record • Coding - $$$
Close • Close counts in atomic bombs • Close counts in horseshoes • Close does not count in coding • If there is no code, then there is no code • Yes, we do bill for Active Duty services (in MSA we bill Coast Guard, in MAC will bill)
5b. Outcome of monthly inpatient coding audit: Inpatient Professional services audited and deemed correct (C.5) NAVY
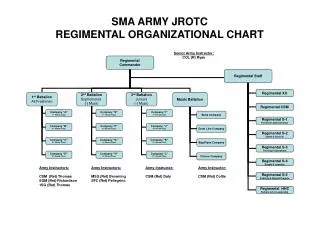
5b. Outcome of monthly inpatient coding audit: Inpatient Professional Services encounters audited/deemed correct ARMY
5b. Outcome of monthly inpatient coding audit: Inpatient Professional Services encounters audited/deemed correct: AIR FORCE
6a. Percentage of outpatient medical records on-hand containing the documentation and/or the loose documentation of the encounter selected to be audited or documented as checked out? (C.6) NAVY
6a. % of outpatient medical records on-hand or documented as checked out? ARMY
6a • Why the variation • Is this a random audit? • Are ALL SADRs for the MTF included • Technicians/nurses • Telephone calls • ALL MEPRS (include FBI) • What qualifies as “checked-out” – in the past week, past month, past year, past decade? • What do the data tell us?
6c. What is the percentage of ICD-9 codes deemed correct? ARMY
6d. Percentage of CPT codes deemed correct? ARMY
Audits • All data included population • Each encounter equally likely to be selected • Random selection of sample from entire population • A person will continue to code in the same manner he has coded unless acted upon by an outside source
Your Commander Signs: 9. I am aware of data quality issues identified by the DQMC Review List and when needed, have taken action to improve the data from my facility.
Objectives • Understand Data Application • Understand What the Data Are and Are Not Indicating • Understand “Random” When Applied to Audits