Download
1 / 71
710 likes | 1.1k Views
Breast. Modified sweat glands. Lobes and lobules of gland in fat tissue stroma. Lactiferous ducts merge just beneath he nipple to form a lactiferous sinus. Then individually open on nipple. Ducts emerge from acini of glands Smaller ducts join to form lactiferous ducts. Lobes and lobules

E N D
Modified sweat glands. • Lobes and lobules of gland in fat tissue stroma. Lactiferous ducts merge just beneath he nipple to form a lactiferous sinus. Then individually open on nipple • Ducts emerge from acini of glands • Smaller ducts join to form lactiferous ducts
Lobes and lobules • of gland in fat tissue stroma. • Ducts emerge from acini of glands • Smaller ducts join to form lactiferous ducts
Axillary A lateral thoracic Internal mammary A perforating Intercostal lateral Axillary vein Internal mammary V Intercostal veins Supraclavicular nerve Itercostal N sympathatic
Benign Breast Disease • Congenital Conditions • Traumatic Conditions • Infections • Aberrations of Normal Development and Involution (ANDI) • Neoplastic • Benign - Fibroadenoma
Congenital Conditions • Congenital • Supernumerary nipple along nipple line • Supernumerary breast • Aplasia – turners, Juvenile hypertrophy
Traumatic Conditions • Traumatic fat necrosis • Cracks of nipple • Hematoma • Traumatic mastitis • Milk fistula
Traumatic Conditions (Fat Necrosis) • Follows trauma, surgery or radiation • Small, hard mass - confused with carcinoma • Focal necrosis of fat with inflammation • Foamy lipid-laden macrophages • Later fibrosis, calcification
Mammary fistula • Congenital (rare) • Acquired • Varient of MDE • Incision and drainage of abcess in lactating breast
Acute Mastitis neonatorum Pubertal mastitis Traumatic mastitis Metastatic mastits Mammary duct ectasia Lactational mastits Acute suppurative mastitis Chronic Chronic non specific chronic breast abscess Hidradenitis Pilonidal Disease Postoperative Wound Infections specific Tuberculosis Syphillis Actinomycosis Infections
Duct Ectasia and Periductal Mastitis • ? Aetiology, age 40s - 50s, smokers • Dilatation of breast ducts - fill with stagnant brown/green secretion - atrophy and loss of ductal epithelium - secretion spills into periductal tissues - inflammatory reaction (‘mastitis’) • Micro - lyphocytes, histiocytes, plasma cells • Secondary anaerobic infection, abscess • Fibrosis - slit-like nipple retraction
DuctEctasia andPeriductal Mastitis • Presentation • Nipple discharge - any colour • Nipple Retraction • Subareolar mass • Abscess • Mammary duct fistula • May mimic carcinoma
Duct ectasia Nipple discharge - any colour Nipple retraction Lump Abscess Mammary duct fistula
Antibiotics • Flucloxacillin & • Metronidaziole • NSAID Central duct excision (Hadfield operation)
Operations - Hadfield’s Major Duct Excision • Indications : • duct ectasia (periductal mastitis) with recurrent episodes +/- fistulae • blood stained discharge from one or more ducts in women > 40 • Incision : • circumareolar but < 3/5 the areolar circumference to allow enough blood supply • include the orifice of any sinus or fistula
Operations - Hadfield’s Major Duct Excision Technique : • cut the subcutaneous tissue down to the ducts • dissect in a plane circumfentially around the terminal lactiferous ducts • divide the ducts close to the nipple and remove with a small conical wedge of tissue • include fistulous tracts with all granulation with excision • +/- DT closure 4/0 subcuticular
Bacterial Mastitis • Cracks and fissures form in early breastfeeding • Secondary infection with Staph. aureus • Carried by nasopharynx of infant • Abscess • Chronic scar
Fever Throbbing pain Skin oedema Aspiration of pus
Operation - Incision & drainage breast abscess • Breast abscess : • most occur during lactation • empty the breast , allowing the baby to feed by the other breast • drain early when there is a point of maximal tenderness - needle aspiration + antibiotics may be more appropriate • Technique : • General anaesthesia • incise • over point of maximal tenderness or fluctuance • if near the nipple use circumareolar incision • deepen the incision until drain pus, send for M/C/S • Use counter incision in upper breast • break down loculations & take Bx (exclude inflam Ca) • +/- DT +/- kaltostat packing • supportive bra, breast feed when comfortable
Operations - Breast Excisional Biopsy • Indication : solid breast lump that is clinically benign • Aim : to extract the lesion with minimal margin and least cosmetic defect to establish a histological Dx and remove the palpable lump.
Breast Excisional Biopsy • Incisions : • incise over the lump - adequate excision 1st priority • 2nd comes aesthetic position • if possible scar hidden by bra • medial incisions more likely to develop keloid • avoid radial incisions except medially • make incision within skin that would be removed if patient subsequently required a mastectomy • Technique : excise lump completely without cutting into it • hold specimen with Lane or Allis tissue forceps • careful haemostasis +/- DT + L.A. • subcuticular closure
Fibrocaseous Caseous form Suppurative form Sclerosing form
Tuberculosis • Antituberculous drugs • Cold abscess • Valvular incision • Local anti TB • Fibrocaseous • Simple mastectomy • Anti TB
ANDI( Fibrocystic Disease) • Developed by LE Hughes at Cardiff 1987 • Replaces fibrocystic disease, fibroadenosis, etc. • Main Histological Features: • Epithelial proliferation • Adenosis (increase in no. of acinar units per lobule) • Epithelial Hyperplasia ( of cells) + Papilloma formation • Fibrosis • Cysts • Retention cysts • Blue –domed cyst of Bloodgood (macrocysts) • Brodie’s tumor (microcysts)
Presentation • Mastalgia • Cyclical • Non-Cyclical • Lump - many causes • Periareolar Disorder • Nipple Discharge • Nipple Retraction
Cyclical Mastalgia • Presentation • Median age 35 yrs • Premenstrual breast discomfort • Upper outer quadrant (often bilateral) • Relief during menstruation • Associated with nodularity • Aetiology presumably hormonal
Non-Cyclical Mastalgia • Not related to menstrual cycle • Median age 45yrs (pre- or postmenopausal) • Unilateral, well-localised, ‘trigger spot’ • Multiple Causes • Carcinoma • Mammary Duct Ectasia • Sclerosing Adenosis (ANDI) • Painful Scar • Musculoskeletal Pain • Mondor’s Disease
Lumps • Traumatic • Fat Necrosis • Organized hematoma • Inflammatory • Mammary Duct Ectasia/Periductal Mastitis • Chronic breast abcess • ANID • Nodularity • Cysts (Galactocele) • Sclerosing Adenosis • Neoplastic • Benign • Lipoma • Hard Fibroadenoma • Giant fibroadenoma • Phyllodes Tumour • Malignant
Nodularity • Often bilateral, upper outer quadrant • May be cyclical • Associated with mastalgia • Histology (ANDI) • Cysts • Fibrosis • Adenosis
Cysts • Common, 30s-40s • Often multiple, bilateral • Present suddenly (fluid) + pain, nodularity • Tense, less mobile than Fibroadenoma • Involution of stroma and epithelium • Turbid fluid (blue) • Apocrine or simple cuboidal epithelial lining
Galactocele • Solitary subareolar cyst • Dates from lactation • Contains milk • Can calcify • Can greatly increase in size
Cysts of the breast Cysts of the breast Ductal system Neoplastic Stroma Skin cysts ANID Galactocele Benign Malignant • Serous • Lymphatic • Blood • Inflammatory • TB cold abscess • Chronic abscess • Hyadatid Sebaceous Dermoid Microcysts Macrocysts Duct papilloma Papillary cystadenoma Degeneration of carcinoma Degeneration of sarcoma Intracystic carcinoma
Nipple Discharge • Physiological - pregnancy/lactation • Duct Ectasia • Galactorrhoea • Duct Papilloma • Carcinoma • Cysts • Idiopathic
Galactorrhoea • Milky discharge unrelated to lactation • Primary Physiological • Menarche • Menopause • Stress • Mechanical Stimulation • Secondary • Drugs: haloperidol, metoclopramide • Increased Prolactin: pituitary tumour, paraneoplastic
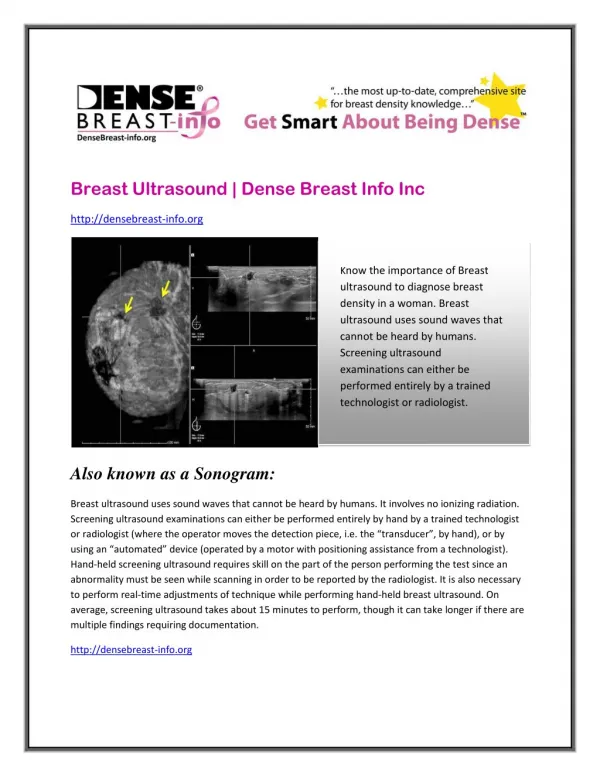
Management of Breast Symptoms • Breast Lump - always need to exclude Ca • Breast examination - Is there a lump or localised nodularity? • Is there no lump or diffuse nodularity? • Triple Assessment • 1. FNA • 2. U/S • 3. Mammography
Breast Lump – Cyst and Mx no lump or diffuse nodularity O/E discrete lump or localised nodularity present FNA solid cystic bloody fluid residual lump then do cytology & mammography no blood no residual lump then no cytology re-examine in 6/12 reassure excisional biopsy
Palpable Breast Lump - Solid Mx FNA solid lump Cytology Mammography > 35 U/S Tru-cut Ò biopsy (lump > 2cm) suspicious or carcinoma Manage as for breast cancer benign Panel comment : If pt 25 - 35 need FNA/ trucut Dx of fibroadenoma otherwise need exc Bx. If tru-cut = normal breast tissue then still need histology of the lump. • observe but excise if : • age >35 • Pt requests • pain • increasing size • equivocal cytology
No Palpable Breast Lump Mx no lump or diffuse nodularity age < 40 age > 40 re-examine 6/52 Cytology Mammography U/S benign benign suspicious or carcinoma reassure reassure Manage as for breast cancer
Nipple discharge Nipple discharge Unilateral Bilateral (multiductal) Multiductal Uniductal Physiological Pathological Fibroadenosis Papillomatosis Duct ectasia Duct papilloma Duct carcinoma Duct ectasia Chronic absces ??? fibroadenosis Fibroadenosis Papillomatosis Duct ectasia ?? carcinoma Mammography U/S Cytology,prolactin,ductography Microdochectomy
Fibroadenoma • Peak incidence 15-25 yrs • Smooth, highly mobile • 2-3 cm occasionally multiple • Benign tumour of fibrous and glandular tissue • Mono- or polyclonal (cyclosporin)