Download
1 / 1
10 likes | 193 Views
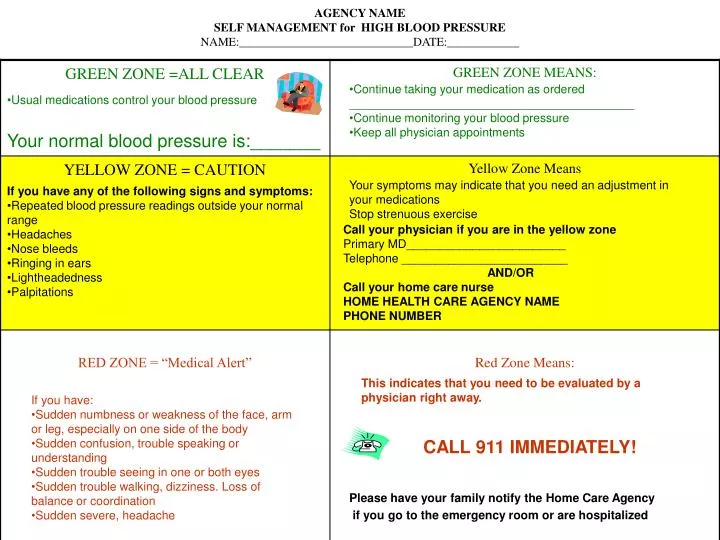
AGENCY NAME SELF MANAGEMENT for HIGH BLOOD PRESSURE NAME:_____________________________DATE:____________. Usual medications control your blood pressure. Continue taking your medication as ordered ___________________________________________ Continue monitoring your blood pressure

E N D
AGENCY NAMESELF MANAGEMENT for HIGH BLOOD PRESSURENAME:_____________________________DATE:____________ • Usual medications control your blood pressure • Continue taking your medication as ordered • ___________________________________________ • Continue monitoring your blood pressure • Keep all physician appointments Your normal blood pressure is:_______ Your symptoms may indicate that you need an adjustment in your medications Stop strenuous exercise • If you have any of the following signs and symptoms: • Repeated blood pressure readings outside your normal range • Headaches • Nose bleeds • Ringing in ears • Lightheadedness • Palpitations Call your physician if you are in the yellow zone Primary MD________________________ Telephone _________________________ AND/OR Call your home care nurse HOME HEALTH CARE AGENCY NAME PHONE NUMBER This indicates that you need to be evaluated by a physician right away. • If you have: • Sudden numbness or weakness of the face, arm or leg, especially on one side of the body • Sudden confusion, trouble speaking or understanding • Sudden trouble seeing in one or both eyes • Sudden trouble walking, dizziness. Loss of balance or coordination • Sudden severe, headache CALL 911 IMMEDIATELY! Please have your family notify the Home Care Agency if you go to the emergency room or are hospitalized