Download
1 / 22
220 likes | 426 Views
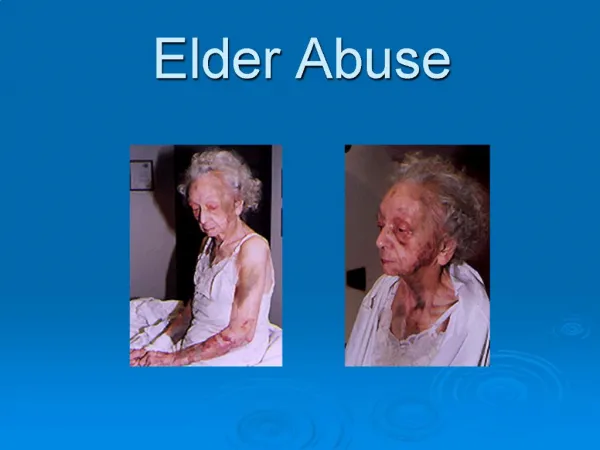
Domestic Violence Interclerkship : Elder Abuse Elizabeth Howard, MD Division of Geriatric Medicine. Definition of Elder Abuse.

E N D
Domestic Violence Interclerkship: Elder AbuseElizabeth Howard, MDDivision of Geriatric Medicine
Definition of Elder Abuse …either harm to a vulnerable elder that occurs because of an intentional act by a caregiver who has a trust relationship with the elder, or a failure of a caregiver to satisfy an elder’s basic needs or protect them from harm. Compiled: The National Academy of Sciences http://www.nasonline.org
Types of Abuse • Physical/Sexual • Psychological • Material/Financial • Neglect • approximately 50% of the cases reported each month in Worcester County • The category of self neglect also investigated by the Department of Protective Services (DPS)
Neglect • Neglect-failure of the caregiver to provide for the basic needs of the elder • Abandonment-desertion of a vulnerable elder • Self neglect-inability of the elder to maintain their basic self care and protection to the point of increased risk of serious harm
Incidence of Elder Abuse • World Health Organization (WHO) found combined rates of elder abuse at 4 - 6 % of the elderly population.* • National Elder Abuse Incidence Study 1998-estimated approximately 550,000 older adults per year are subject to abuse. • Actual number of cases is thought to be much higher due to under reporting - in both the community and institutional settings. *WHO data include Finland, Great Britain, and the United States
Local Statistics on Elder Abuse • The Worcester Department of Protective Services reports that approximately 120 cases of elder abuse are reported each month in this city and immediate surrounding towns. • Of those, approximately 90 (75%) fit the criteria for DPS investigation • Of those, approximately 1/3 require a case to be opened. • Approximately 50% are cases of neglect. • 90% of the cases the abuse is from a family member (spouse or adult child).
Barriers to Detection of Elder Abuse • Reluctanceor inability of the victim to report abuse e.g. Elder may have dementia, feel ashamed, or frightened • Reluctance of the healthcare provider to screen vulnerable elders • Health care providers lack of comfort with reporting their findings • Isolation of the victims University of Nebraska Medical Center http://www.nebraskamed.com/Health-Library/6791/Conditions-AZ-Domestic-Violence
Vulnerable Elder: Who is at risk? • 75 yrs./frail/w>m • Cognitive impairment/dementia with behaviors • Financial stressors – especially caregiver dependence on elder’s money • Caregiver with history of • Drugs • Alcohol • Mental illness • Family dysfunction • Family hx. of domestic violence • Social isolation • Elderly caregiver • (e.g., spouse)
May not be emotionally or physically able to provide consistent care May lack education about the patient’s medical needs/disease progression May not be able to handle the behavioral complications of dementia May not have support of other family members/criticized /no relief May develop depression, anxiety, anger, feel isolated in the caregiver role May not ask for help in time Caregiver Crisis
Screening all Elders Interview the patient without the caregiver at some point during the encounter. Notice if the caregiver is reluctant to leave or does not let the elder speak for themselves. Ask yourself: Are the needs of this elder being met? Ask the patient: Is there any difficult behavior in your family you would like to tell me about? [or] How are things at home? [or] Do you feel safe at home? University of Nebraska Medical Center http://www.nebraskamed.com/Health-Library/6791/Conditions-AZ-Domestic-Violence
When Interviewing a Patient • Be an active listener, good eye contact, be patient for their responses. • Ask open ended questions and follow up with more specific topics if increased concern. • Be nonjudgmental and let them know you have concern for their situation. • Offer resources/safety plans. • Document physical and cognitive findings
Red Flags in the History History is inconsistent with physical exam Conflicting accounts from patient and caregiver Failure of response to usual therapy Frequent use of the ER, or multiple clinics/hospitals Delay in presentation for treatment Pt. not allowed to speak for themselves, even if capable A history of alcohol or drug abuse in the elder or their caretaker University of Nebraska Medical Center http://www.nebraskamed.com/Health-Library/6791/Conditions-AZ-Domestic-Violence
Physical Exam Red Flags Atypical patterns of injury Multiple injuries Injuries at different stages of healing Burns may be suspicious if not well explained Malnutrition not due to an underlying disease Dehydration not due to an acute illness Poor hygiene Infestations with multiple excoriated lesions Pressure Ulcers Perineum bruising or vaginal/rectal trauma University of Nebraska Medical Center http://www.nebraskamed.com/Health-Library/6791/Conditions-AZ-Domestic-Violence
Autonomy vs. Self Neglect • Determining the patient’s decisional capacity is the critical factor. • There is no one diagnostic tool to determine capacity. • Start with your interview, neurologic exam and cognitive assessment (e.g. the mini-cog test or the MMSE). • Gather collateral information from: home health, nursing and family.
Determining Decisional Capacity • Can the patient make/express personal preferences? • Can the patient comprehend risk vs. benefit of their decisions? • Does the patient understand the implications? • Can the patient provide reasons that are rational for their alternative decisions? American Geriatrics Society (AGS) http://www.americangeriatrics.org/
The Role of the Health Care Provider Keep your mind open to the potential of elder abuse Clarify the elder’s functional status (ADLs & IADLs) and physical or sensory safety impairments Clarify living situation: who is in the home social support/services Look for inconsistencies in the hx. vs. the exam findings, get needed lab or xrays Document clearly the patient’s decisional capacity Obligated to report suspected cases to the DPS
Frequent Reasons Elders Decline the DPS • Fear of having to leave their home • Desire to protect their caregiver from legal action • Distrust/unfamiliar with available services • Family history of dysfunction and elder’s needs have added increased stress • Elder’s cognitive decline may go unrecognized/ undocumented • Elder viewed as “ competent” Worcester Department of Protective Services http://www.eswa.org/protective_services/default.cfm
Department of Protective Services • Mandated reporters have immunity from any civil or criminal liability that results from making the report. • Massachusetts State Law requires physicians, nurses, social workers, dentists, police, firefighters, council of aging employees, and assisted living personnel to report these cases to the Department of Elder Affairs. The Massachusetts District Attorneys Association http://www.mass.gov/?pageID=dmdaterminal&L=2&L0=Home&L1=Mandated+Reporting&sid=Dmdaa&b=terminalcontent&f=mandated_reporting_elder_abuse&csid=Dmdaa
Department of Protective Services • They are obligated by law to contact the elder and notify them that there has been a concern expressed. • If the elder has been evaluated as having decisional capacity and they refuse services the case is closed. • Court ordered services must be sought for abused elders who are unable to make informed decisions, and are at risk of serious harm. • If serious abuse is confirmed protective services makes a report to the D.A. office for possible prosecution. Office of Elder Affairs http://www.eswa.org/
Response Plan • The Elder Services of Worcester Protective Services Program can offer assistance in a step wise fashion to the elder with access to multiple agencies and services. • They will officially notify the Health Care Provider of the status of the case by mail. • The Health Care Provider can stay in contact with Elder Services to help monitor the patient’s status.
Resource URLs American Geriatrics Society (AGS) http://www.americangeriatrics.org/ Massachusetts District Attorneys Association http://www.mass.gov/?pageID=dmdaterminal&L=2&L0=Home&L1=Mandated+Reporting&sid=Dmdaa&b=terminalcontent&f=mandated_reporting_elder_abuse&csid=Dmdaa National Academy of Sciences (NAS) http://www.nasonline.org Office of Elder Affairs http://www.eswa.org/ University of Nebraska Medical Center http://www.nebraskamed.com/Health-Library/6791/Conditions-AZ-Domestic-Violence Worcester Department of Protective Services (WPS) http://www.eswa.org/protective_services/default.cfm World Health Organization (WHO) http://www.who.int/en/
Acknowledgements Colleen Burnham*, MBA, Office of Educational Affairs, UMMS Donald W. Reynolds Grant Program for Advancing Geriatrics Education. Jerry Gurwitz, MD, Chief, Division of Geriatric Medicine, UMMS Donald W. Reynolds Grant Co-principal Investigator Julie Jonassen*, PhD, Associate Professor, UMMS School of Medicine, UMMS Graduate School of Biomedical Sciences Mary Ellen Keough, MPH, Office of Educational Affairs, UMMS Donald W. Reynolds Grant Program for Advancing Geriatrics EducationProject Manager Sarah McGee*, MD, MPH, Director of Education for the Division of Geriatric Medicine, UMMS Donald W. Reynolds Grant Director of the Advancing Geriatrics Education Resource Center Erika Oleson*, DO, MS, UMMS Donald W. Reynolds Grant Clinician Educator in the Division of Geriatric Medicine Susan Pasquale, PhD, Director of Curriculum & Faculty Development in the Office of Faculty Affairs, UMMS Donald W. Reynolds Grant team member Michele Pugnaire*, MD, Senior Associate Dean for Educational Affairs, UMMS Donald W. Reynolds Grant Co-principal Investigator *author