Download
1 / 19
190 likes | 339 Views
A case of psychiatric drug D.O. Clinical Toxicology Course Dr. Cynthia Shum UCH AED. History. A 44-yr lady was brought in at 7:30pm by ambulance Suicidal attempt Took 20 tabs of drugs from 10am to 3pm and 10 tabs of another drug at 3pm. Vital signs:. BP 101/70 Pulse 69/min Temp. 36.5

E N D
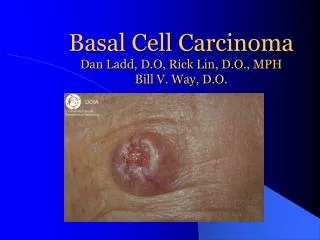
A case of psychiatric drug D.O. Clinical Toxicology Course Dr. Cynthia Shum UCH AED
History • A 44-yr lady was brought in at 7:30pm by ambulance • Suicidal attempt • Took 20 tabs of drugs from 10am to 3pm and 10 tabs of another drug at 3pm
Vital signs: • BP 101/70 • Pulse 69/min • Temp. 36.5 • RR 20/min • SpO2 100% on RA
Physical Examination • GCS 15/15, pupils 3-4mm reactive • Skin normal, bowel sound normal, no bladder • Patient was upset, lethragic, tremor of hands was noted, but no weakness, no fasciculation, jerks not hyperactive
Bedside Investigation • H’stix 3.5 • ECG: SR normal QRS, QTc 0.46sec
PMH: • Bipolar depression FU YFS • On Lithium SR and clonazepam. • Empty bags of Lithium SR (400mg/tab) and clonazepam (1mg/tab) found • Total ingestion: Lithium SR 20tabs x 400mg = 8 gm Clonazepam 10tabs x 1mg = 10mg
Investigations: Li level RFT Paracetamol/salicylate CBP INR AXR Decontamination Lavage AC Forced diuresis WBI: PEG 2L/hr until clear return What is your management?
Supportive Fluid and electrolyte Adequate Hydration IVNS for good urine o/p Foley to BSB What’s your management?
Blood results: • Li level 4.2mmol/L • RFT normal • Na, K normal • CBP, INR normal • Paracetamol/salicylate negative • AXR: no tablets seen What else would you do?
Progress: • ICU admission • HD started 200-250ml/min x 3 hrs • Patient was closely monitored and given bolus of fluid to maintain BP during HD
Acute Toxicity Action Level WBI Chronic Toxicity Time (Hour) From time of AED attendance HD HD
Lithium Sustained-Release • Absorption: • Delayed for 6-12 hrs, completed for another 8hrs • Distribution • Vd 0.6-0.9L/kg, Rapidly to blood, liver, kidney • Metabolism • Nil • Elimination • 95% by kidneys, minority by sweat & saliva • T1/2 20-24hrs
Clinical manifestation • No/mild GI symptoms in SR form • CNS: Mild: weakness, fine tremor, light headedness Moderate: muscle twitching, tinnitus, hyperreflexia, slurred speech, drowsiness, apathy Severe: confusion, clonus, choreoathetoid movement, seizure, coma
Acute on chronic toxicity • CNS symptoms exclusively • High total body burden of Li in chronic use • Additional increase results in immediate toxicity • Predisposing factors • Continuation of high dose after acute mania • Na restriction • Intravascular volume depletion • Decreased GFR • Drug interation: NSAID, ACEI, SSRIs, antipsychotics
Laboratory testing • RFT • Look for the etiology of toxicity • Predict response to conservative Rx • Serial Li level • Monitor response to therapy • Reference • Therapeutic level: 0.6-1.2 mmol/L • Action level for acute toxicity: >4 mmol/L • Action level for chronic toxicity: >1.5 mmol/L
Haemodialysis • Who should get HD? • When to initiate HD? • Those who are initially poisoned and have high Li levels but no S/S of may benefit the most After Li has distributed the CNS, if is more difficult to remove by HD and permanent sequelae may occur
Who and when to HD? • Symptoms • Significant neurological symptoms • Level • Acute ingestion with Li >4mmol/L • Acute on chronic with Li >1.5 mmol/L • Failure of excretory pathway • Renal failure • Intolerable to Na repletion, e.g. CCF
Rebound Li level • HD clears only the plasma • Significant Li load in tissue • Levels • Immediate and 6hrs post HD • Look for rebound
Thank you Q & A

![[PDF] DOWNLOAD Drug-Drug Interactions With an Emphasis on Psychiatric Medications](https://cdn7.slideserve.com/12495694/slide1-dt.jpg)
![[READ DOWNLOAD] Drug-Drug Interactions With an Emphasis on Psychiatric Medications](https://cdn7.slideserve.com/12515349/slide1-dt.jpg)