Download
1 / 12
120 likes | 337 Views
Lynch Syndrome Case Study. Louise Bourdon, KGC. Patient MF. Referred in 2003 aged 55 (by Family Cancer Clinic at St Mark’s Hospital) Colon cancer aged 37 Caecal cancer in her 40s Oesophageal cancer in her 50s Family history of CRC Daughter died at 32yrs of age Lung metastases

E N D
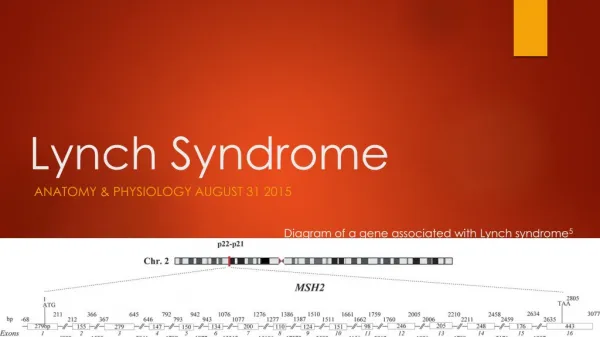
Lynch Syndrome Case Study Louise Bourdon, KGC
Patient MF • Referred in 2003 aged 55 (by Family Cancer Clinic at St Mark’s Hospital) • Colon cancer aged 37 • Caecal cancer in her 40s • Oesophageal cancer in her 50s • Family history of CRC • Daughter died at 32yrs of age • Lung metastases • Primary tumour in bowel
Investigations Performed • Mutation screening of MLH1 and MSH2 genes • DGGEof all exons, and sequencing of any shifts • No mutation identified - Reported in October 2003 • IHC performed at University College London Hospitals • Loss of MSH2 and MSH6 • Followed by microsatellite studies at KGC - unstable • Suggestive diagnosis of Lynch - Reported May 2004 • MSH6 Mutation screen • DGGE of all exons, and sequencing of any shifts • No mutations identified - Reported September 2005 • MLPA for MLH1 and MSH2 also reported (MRC-Holland kit P003) • MSH6 MLPA (MRC-Holland kit P008) • Normal for MSH6 - Reported November 2006 • ?Heterozygous deletion of probe upstream of MSH2
Contact With MRC-Holland • July 2006 - Member of staff contacted MRC-Holland following apparent heterozygous deletion of one probe in the P008 kit (EPCAM probe – 15kb upstream of MSH2) • MRC-Holland emailed laboratory in December 2008 • Emailed reference of Nature Genetics paper1 • Discussed mechanism behind deletion and loss of MSH2 • Announce new probes in kit P072 being released in early 2009
EPCAM deletion analysis • Review of patients with loss of MSH2/MSH6 not originally screened with kit P072 • 5 patients screened • One patient clearly positive (MF) • Second patient failed quality control measures but appeared heterozygous for deletion • Second laboratory investigating same patient using long-range PCR confirmed presence of mutation • Recently confirmed MSH2 promoter methylation for both patients using MS-MLPA kit (ME011)
EPCAM deletions • Families identified with deletions of last exon of EPCAM gene (originally called TACSTD1) • Two deletions identified to date • c.859-1462_*1999del in Dutch population1 • C.555+894_*14164del in Chinese population1 • Gene is directly upstream of MSH22 • Deletion includes polyadenylation signal and results in the transcription read-through into MSH2 • Promoter of MSH2 on same allele is methylated (can be detected using MS-MLPA kit (MRC-Holland kit ME011) • Loss of expression of MSH2 (resulting in negative IHC for MSH2 and MSH6)
EPCAM Deletion Families • One study noted that the phenotype for their cohort of EPCAM deletion families differed slightly from “classical” Lynch families3 • Diagnosed almost exclusively with CRC • MSH2 mutation carriers more frequently develop extracolonic tumours • Important to note that this is not reproducible in all studies
Promoter Hypermethylation • MLH1 promoter hypermethylation is a known phenomenon • Some cases show germline methylation (~5% MLH1 negative IHC patients) • MSH2 promoter hypermethylation known to segregate with EPCAM deletion • Only somatic cases identified (~6% MSH2 negative IHC) • No promoter methylation identified in lymphocyte DNA (possibly result of low levels of EPCAM transcription in this tissue2)
References • Ligtenberg, M.J. et al (2009) Heritable somatic methylation and inactivation of MSH2 in families with Lynch syndrome due to deletion of the 3’ exons of TACSTD1 Nat Genet41(1):112-117 • Niessen, R.C. et al (2009) Germline Hypermethylation of MLH1 and EPCAM deletions are a frequent cause of Lynch syndrome Genes, Chrom & Cancer48:737-744 • Kovacs, M.E. et al (2009) Deletions removing the last exon of TACSTD1 constitute a distinct class of mutations predisposing to Lynch syndrome Hum Mutat30:197-203