Download
1 / 47
470 likes | 586 Views
A Risk Prediction Model for Recurrent Events in Chronic Coronary Heart Disease: The Heart and Soul Study. Ivy Ku, Eric Vittinghoff, Kirsten Bibbins-Domingo, Michael Shlipak, Mary Whooley January 14, 2011. Background and Significance. 1 in 3 Americans live with cardiovascular disease

E N D
A Risk Prediction Model for Recurrent Events in Chronic Coronary Heart Disease: The Heart and Soul Study Ivy Ku, Eric Vittinghoff, Kirsten Bibbins-Domingo, Michael Shlipak, Mary Whooley January 14, 2011
Background and Significance 1 in 3 Americans live with cardiovascular disease With advances in therapies, patients live longer with CHD Prognosis varies widely Risk stratification integral to patient management
Risk Prediction in Primary Prevention 10-year risk of incident coronary heart disease (CHD) Guides cholesterol and BP treatment in primary prevention
Predictors of worse outcomes in stable CHD Biomarkers: CRP, BNP, hs-troponin
Risk Prediction in Stable CHD Clinically useful, up to date, simple, integrated risk scores lacking HERS, LIPID, Framingham severe limitations Furthermore, long-term risk in CHD has not been well-characterized and quantified CHF not included in CHD risk prediction
Project Aims To develop a clinical prediction model and point score for 5-year risk of recurrent CV events in stable CHD To quantify and categorize the range of long-term risk in stable CHD
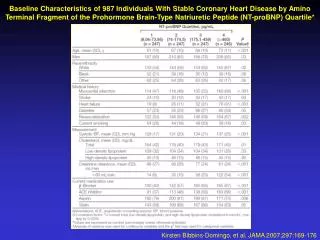
Methods • The Heart and Soul Study • Cohort study of 1024 subjects with stable CHD enrolled 2000-02 • Effect of psychosocial factors on prognosis in stable CHD • Thorough phenotyping of baseline condition, biomarkers, echo, stress • Mean 6 years follow-up, > 400 CV events
Population SF bay area VA, UCSF, CHN clinics Inclusion: hx MI, revascularization, angiographic CAD, abnormal stress test Exclusion: MI within 6 mo, unable to walk 1 block, moving away within 3 years
Methods • 2 Cox models • Dichotomized predictors • Continuous predictors • Composite outcome: time to MI, CVA, CHF hospitalization, or CV death • Use baseline survival function, relative hazards to calculate 5-year risk
Coding of Predictors • Selected functional form of continuous predictors using AIC • categorical (quantiles, clinical cutpoints) • linear • 3, 4, 5 knot restricted cubic splines • Steyerberg recommends doing this a priori if possible, to avoid over-fitting • Cross-validation can also be used
Model selection • Need to maximize the signal without over-fitting • Three main strategies: • Outcome-free data reduction: use the literature, expert opinion, practical considerations to eliminate candidate predictors without looking at the outcome • Parsimony: select highly significant predictors • Cross-validation (CV): mimics external validation
Our implementation Outcome free data reduction: eliminated 18 of 36 candidate predictors on the basis of expert judgment, practical considerations Parsimony: cut 4 more using backward selection Cross-validation: 10-fold CV of C-index for ~1,000 candidate models Final decision between top candidates again considered clinical convenience and face validity
How cross-validation works • Divide sample into 5-10 subsets • For each subset: • set aside, fit model to remaining subsets • calculate predictions for set-aside subset • Estimate prediction error using quasi- external predictions for all observations • Repeat ~20 times and average results • repetition needed to reduce noise
C-index A measure of model discrimination Extension of C-statistic, area under ROC curve to survival models Estimates probability that in a randomly selected pair of observations, the earlier failure has the higher predicted risk Naïve C-index is optimistic; cross-validation reduces the optimism
Selecting Point Score Model • Cross-validation involves five steps for each candidate point score model: • fit model using binary predictors only • round coefficients to obtain point scores • refit model using calculated point scores as sole (continuous) predictor • save predictions from the refitted model • use predictions to calculate CV C-index
Shrinkage using calibration slope • Cross-validation to get calibration slope: • calculate xb for omitted subsets • re-fit model using xb as the sole predictor • coefficient for xb <1.0 signals over-fitting • Use slope to improve calibration • shrink coefficients by calibration slope (i.e., the coefficient for xb in the refitted model) • pulls in extreme high and low predictions • does not affect discrimination
Model Performance • Discrimination: C-index • Net reclassification improvement (NRI) • continuous vs point score models • continuous model vs Framingham • Calibration: goodness-of-fit test, visual inspection, calibration slope
External Model Validation • Cross-validation is strictly internal • reduces over-fitting • but does not protect against predictor effects that differ across populations • Plan external validation in separate cohort • recommended by Altman and Royston, often demanded by reviewers
Functional Form Determined by AIC Age linear LVEF dichotomized at 50% UACR, BNP, BMI, CRP: 3-knot restricted cubic splines
Backward Selection • Eliminated 4 weakest predictors (p>0.5) • HDL, LDL, hx MI, HTN • Top 4 predictors were always the same by all exploratory methods • Age, EF, BNP, UACR • Remaining 10 candidates • Gender, BMI, smoker, diabetes, CRP, CKD, troponin, hx CHF, med nonadherence, physical inactivity
Screening models using CV Base model age, LVEF, BNP, UACR Screened all 5 to 11-predictor models using 20 repetitions of 10-fold cross-validated C-index Targeting 5 to 7 predictor range, for practicality Done for both point score and continuous models
Final Model • Age, LVEF, BNP, UACR, smoker • Point score • Naïve C-index 0.742 • CV C-index 0.736 • Continuous model • Naïve C-index 0.768 • CV C-index 0.763
Point score Age ≥ 65 1 Smoker 1 LVEF < 50% 2 BNP > 500 3 UACR ≥ 30 3
Calibration Continuous Model Pseudo-Hosmer-Lemeshow goodness-of-fit test: p = 0.94 Cross-validated calibration slope = 0.94
NRI with FHS model 93 cases moved up 47 cases moved down 46 net cases 46 / 243 =18.9%, p < 0.001 329 non-cases moved down 82 non-cases moved up 247 net non-cases 247 / 661 = 37.4% p < 0.001 Net reclassification = 56.3%, p < 0.001
NRI comparing point to cont. 54 cases moved up 29 cases moved down 25 net cases 25 / 246 =10.2%, p = 0.006 153 non-cases moved down 94 non-cases moved up 59 net non-cases 59 / 670 = 8.8% p = 0.002 Net reclassification = 19%, p < 0.001
Summary of results • Our model had good discrimination (CV C-statistic 0.76), and had 56% net reclassification vs framingham secondary events model • Many traditional risk factors (HTN, lipids, obesity) were not significant predictors
Limitations Population (VA men, CHN, urban) No external validation yet
Conclusion Developed a risk model with 5 predictors Can stratify 5-year recurrent CV event risk in stable CHD
External Validation • PEACE cohort • Clinical trial of trandolapril vs placebo in low-risk stable CAD • 3600 subjects with biomarkers • Patients were less sick, excluded EF<40% • 1996-2000
References Steyerberg E. Clinical Prediction Models: A practical approach to development, validation and updating. Springer, NY 2009. Lloyd-Jones D. Cardiovascular risk prediction: Basic concepts, current status, and future directions. Circ 2010; 121: 1768-77. Morrow D. Cardiovascular risk prediction in patients with stable and unstable coronary heart disease. Circ 2010; 121: 2681-91. D’Agostino R. Primary and subsequent coronary risk appraisal: new results from the Framingham study. AHJ 2000; 139: 272-81. Altman DG, Royston P. What do we mean by validating a prognostic model? Stat Med, 2000;19:453-473.