Download
1 / 36
360 likes | 486 Views
CFAR Clinical and Translational Core. Partnership and Collaboration Vision for our Future Dr. Kathy Anastos. Big(gest) picture—Einstein/Montefiore Where we sit in big picture Details of each component What we need to accomplish by May Timeline.

E N D
CFAR Clinical and Translational Core Partnership and Collaboration Vision for our Future Dr. Kathy Anastos
Big(gest) picture—Einstein/Montefiore • Where we sit in big picture • Details of each component • What we need to accomplish by May • Timeline
Keeping our eyes on the PrizeAll biomedical research has as its ultimate goal improving the public’s health Especially if funded with public money
Einstein Research Informatics IT Infrastructure (Network, Storage, Computational Cycles, Security) Informatics Analytics Data integration, Contextualization Data collection Data management Universal Consent For biorepositing of “remainders”
Why Informatics? • Healthcare environment (research, practice, operations) • Increasingly information intensive • Rapidly growing and competitive • Robust informatics and analytic infrastructure critical • The winners will be those using health information processing technologies in more creative and innovative ways 6
Guiding Principles • Learning Healthcare System: • Evidence based • Continuous improvement • Patient Centered • Outcome driven • Precision Medicine: • Personalized Medicine • Clinical Genomics • Epigenomics • Behavioral and Environmental
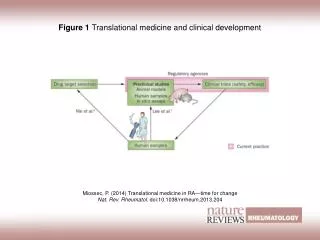
Basic Science Clinical Practice Clinical Research Health Services Research Biospecimens slide idea inspired by Eric Newmann: Translational Medicine from SW Perspective, June 2006 Parsa Mirhaji
Practice Research Transformational Informatics Platform slide idea inspired by Eric Newmann: Translational Medicine from SW Perspective, June 2006 Parsa Mirhaji
Comparative Effectiveness Research Translational Research Personalized Medicine Secondary Use Risk Assessment Data mining, business intelligence Integrated Perspective Fraud Detection Public Health Parsa Mirhaji Mobile Health Decision Support
E/M Research Informatics Basic Science Clinical Research Clinical Practice Operations Genomics Personalized Medicine Guidelines & Best Practices Clinical Trials Patient Empowerment Meaningful Use Rare Diseases Comparative Effectiveness Study Prospective Studies Proteomics Decision Support Multi-institutional Collaborative Research Quality & Outcomes Research Patient Safety, Clinical Error Drug Discovery Biomarkers P4P Health Economy Population Health
Motivations Health Economy CER, PCOR, P4P, HSR Precision Medicine Precision Medicine Bio Repository
Health Economy/ Finance RHIO (Bronx, NY) Community, Environment (Bronx, NY) ACO Bio Repository
Value Of This Infrastructure to CFAR-Both Actual and Perceived • Extant large resource • Montefiore’s strengths become our strengths: community focus, integrated system of care, large investment in IT; leader in IT and CQM/CQI • Grounds us in a large and stable infrastructure • We can be integrated into each component • Brings us control groups, not only in data, but also with tissue and specimens • Creates perception (and reality) of an integrated system
First box—Electronic Health Records • Montefiore’s full clinical set of clinical records • Can identify those HIV+, known HIV-negative, and unknown HIV serostatus • Creates enormous power epidemiologically, and ability to define control groups • Challenges: clinical data is “dirty” and incomplete • How to define the HIV+ population for our data warehouse?
Clinical Populations • Center for Positive Living (ID Clinic) 2980 • CICERO (MMG2, community based) 856 • MMG 1 (MAP) ~250 • Private practices (MAP) ~450 • Division of Substance Abuse (DOSA, 3500) ~700 • Adolescents • Gynecologic practices • HIV+ pregnant women 85 • Montefiore and Bronx Lebanon • Pediatric pre-adolescents • HIV-exposed, uninfected children
Figure 1. Viral Load by CD4 by ARV Medication. Clicking on any number in this table will drill down further and list the cohort with more explicit clinical information
Figure 2. Medication Prescription Year by Discontinuation Year. Clicking on any category of Medication will further drilldown to specific medication (Figure 3).
Current Research Infrastructure • Center for Positive Living • 5 study coordinators • Separate space contiguous to the clinic • Have completed 31 trials, with ~2300 participants • Currently have 16 active studies, 400 participants • Able to recruit rapidly for • translational studies • Behavioral studies • Clinical studies including RCT • Can enroll participants from other sites
Current Research InfrastructureDivision of General Internal Medicine • Extensive junior investigator development with multiple K awards • Bring an unusual strength in substance use • Extensive research in substance use and HIV • 4 R01s (Arnsten, Cunningham, Litwin) • K23 (Litwin) • R03 (Litwin) • CFAR pilot study (Nahvi)
Tasks and TimelineClinical Programs • Create the “join” for the clinical (EHR) database (who are the patients, what are the variables)—Late January • Create program to “pull” the data into a central data warehouse—mid to late February • Develop/expand clinical research groups-January • Consider subgroups of CAB--February • Perform at least two translational studies NOW • Ramp up enrollment into biorepository from clinical populations—begin by late January
How to Expand Biorepository • Expand clinical sites from which can recruit • Expand clinical criteria for enrollment • Expand collection sites: at which enrollment process can occur • Expand types of specimen collected • Overcome other barriers—e.g. restriction on number of enrollees per day for specimen processing • This MUST happen— rapid enrollment
Research Programs (with and without biorepositories) • Women’s Interagency HIV Study (WIHS) • Rwanda Women’s HIV Study (RWISA) • Herold lab’s studies (20 studies, a few hundred patients) • Mark Einstein’s clinical trials/studies • Laurie Bauman’s behavioral studies • Other international populations • These represent not only patients and specimens, but also INFRASTRUCTURE
Some WIHS Specifics • WIHS HPV studies, molecular epidemiology: Howard Strickler and Robbie Burk • WIHS cardiovascular studies: Robert Kaplan • WIHS neurocog studies: led by Chicago WIHS • WIHS body composition and bone studies—led by Bronx WIHS • Extensive established collaborations with other institutions • Local and National specimen repositories: 3 million aliquots: serum, plasma, PBMC, cell pellets, DNA, CVL, vaginal and cervical swabs, urine, saliva, some tissue
Tasks and Timeline—Research Programs with Biorepositories • Identify all existing databases • Researchers provide information on variables and data structure to data team • Prioritize inclusion • Consolidate the research databases from all sources • Perform at least two translational studies NOW
Performing Translational Studies • Requires a COLLABORATION • In other words, the Clinical Core alone cannot create the translational studies • Bench scientists must start using human specimens
So, Concretely, by May • Develop data warehouse from EHRs, and perform at least one epi study • Develop the research data warehouse linked to biorepositories, and perform at least two translational studies • Develop stronger institution-wide ties to DOSA • Rapidly enroll into the clinical services biorepository and perform a translational study • Repackage our strengths
Team(s) • Kathy Anastos—Director of CTIC • Co-Directors: • Julia Arnsten: Clinical and Epidemiologic • Betsy Herold: Translational • Others • Barry Zingman—CPL, integrated research infrastructure • Chinazo Cunningham—community focused research • Data team: Mindy Ginsberg, Marty Packer, Alex Peshansky, (Parsa, Eran) • Others TJ
When our minds can conceive it And our hearts can perceive it Then our hands can achieve it i.e. We can Succeed