Download
1 / 1
10 likes | 125 Views
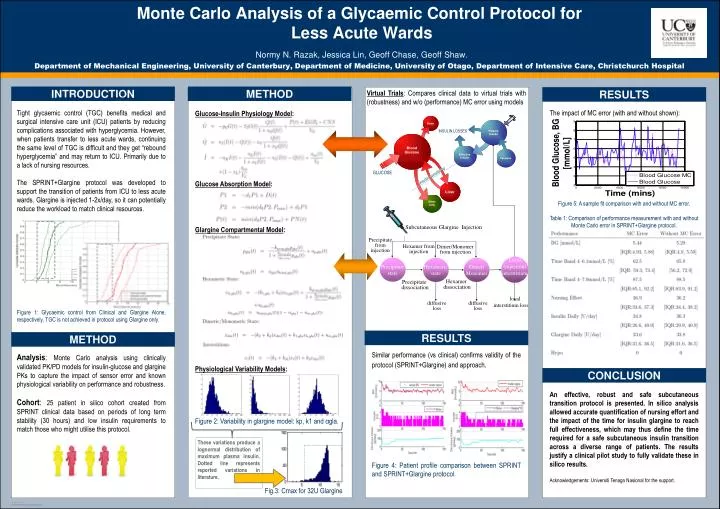
Subcutaneous Glargine Injection. Hexamer from injection. Dimer/Monomer from injection. Local (injection) interstitium. Precipitate state. Hexameric state. Dimer/ Monomer. Hexamer dissociation. Precipitate dissociation. diffusive loss. diffusive loss.

E N D
Subcutaneous Glargine Injection Hexamer from injection Dimer/Monomer from injection Local (injection) interstitium Precipitate state Hexameric state Dimer/ Monomer Hexamer dissociation Precipitate dissociation diffusive loss diffusive loss Monte Carlo Analysis of a Glycaemic Control Protocol for Less Acute WardsNormy N. Razak, Jessica Lin, Geoff Chase, Geoff Shaw.Department of Mechanical Engineering, University of Canterbury, Department of Medicine, University of Otago, Department of Intensive Care, Christchurch Hospital INTRODUCTION METHOD RESULTS Virtual Trials: Compares clinical data to virtual trials with (robustness) and w/o (performance) MC error using models Tight glycaemic control (TGC) benefits medical and surgical intensive care unit (ICU) patients by reducing complications associated with hyperglycemia. However, when patients transfer to less acute wards, continuing the same level of TGC is difficult and they get “rebound hyperglycemia” and may return to ICU. Primarily due to a lack of nursing resources. The SPRINT+Glargine protocol was developed to support the transition of patients from ICU to less acute wards. Glargine is injected 1-2x/day, so it can potentially reduce the workload to match clinical resources. Figure 1: Glycaemic control from Clinical and Glargine Alone, respectively. TGC is not achieved in protocol using Glargine only. Analysis: Monte Carlo analysis using clinically validated PK/PD models for insulin-glucose and glargine PKs to capture the impact of sensor error and known physiological variability on performance and robustness. Cohort: 25 patient in silico cohort created from SPRINT clinical data based on periods of long term stability (30 hours) and low insulin requirements to match those who might utilise this protocol. The impact of MC error (with and without shown): Figure 5: A sample fit comparison with and without MC error. Table 1: Comparison of performance measurement with and without Monte Carlo error in SPRINT+Glargine protocol. Glucose-Insulin Physiology Model: Glucose Absorption Model: Glargine Compartmental Model: Physiological Variability Models: Figure 2: Variability in glargine model: kp, k1 and αgla. Fig.3: Cmax for 32U Glargine INSULIN LOSSES GLUCOSE Precipitate from injection local interstitium loss RESULTS METHOD Similar performance (vs clinical) confirms validity of the protocol (SPRINT+Glargine) and approach. Figure 4: Patient profile comparison between SPRINT and SPRINT+Glargine protocol. CONCLUSION An effective, robust and safe subcutaneous transition protocol is presented. In silico analysis allowed accurate quantification of nursing effort and the impact of the time for insulin glargine to reach full effectiveness, which may thus define the time required for a safe subcutaneous insulin transition across a diverse range of patients. The results justify a clinical pilot study to fully validate these in silico results. Acknowledgements: Universiti Tenaga Nasional for the support. These variations produce a lognormal distribution of maximum plasma insulin. Dotted line represents reported variations in literature.