Download
1 / 1
10 likes | 195 Views
Treatment readiness and cognitive functioning within a therapeutic community H.Kilbane, University of Surrey & HMP Grendon; E. Glorney, University of Surrey; R. Shuker, HMP Grendon. INTRODUCTION

E N D
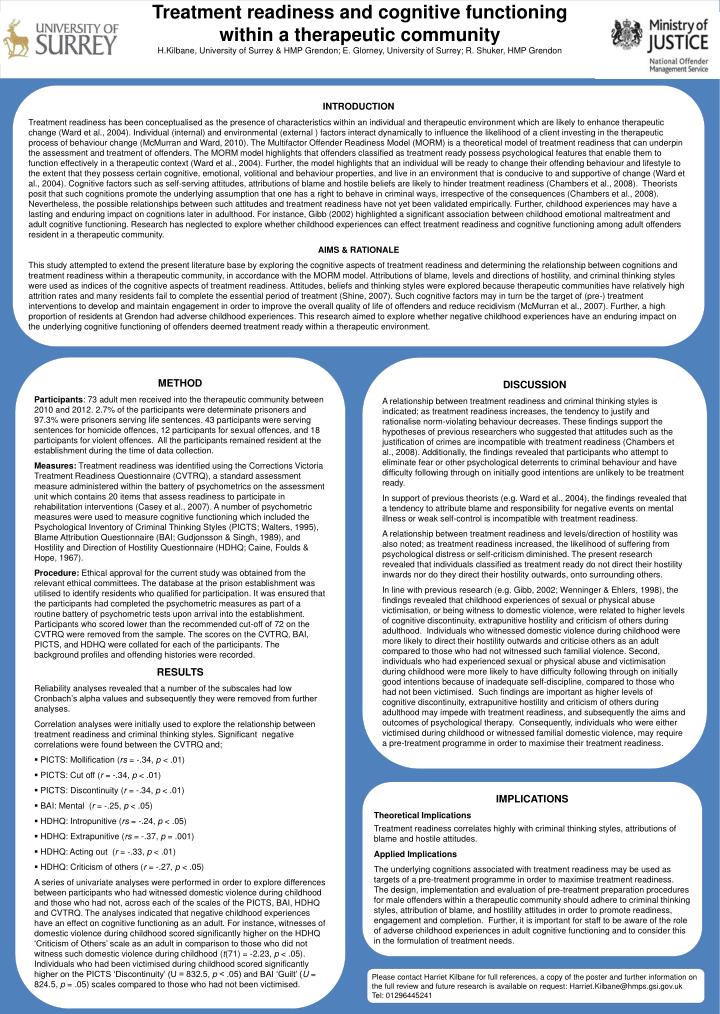
Treatment readiness and cognitive functioning within a therapeutic community H.Kilbane, University of Surrey & HMP Grendon; E. Glorney, University of Surrey; R. Shuker, HMP Grendon INTRODUCTION Treatment readiness has been conceptualised as the presence of characteristics within an individual and therapeutic environment which are likely to enhance therapeutic change (Ward et al., 2004). Individual (internal) and environmental (external ) factors interact dynamically to influence the likelihood of a client investing in the therapeutic process of behaviour change (McMurran and Ward, 2010). The Multifactor Offender Readiness Model (MORM) is a theoretical model of treatment readiness that can underpin the assessment and treatment of offenders. The MORM model highlights that offenders classified as treatment ready possess psychological features that enable them to function effectively in a therapeutic context (Ward et al., 2004). Further, the model highlights that an individual will be ready to change their offending behaviour and lifestyle to the extent that they possess certain cognitive, emotional, volitional and behaviour properties, and live in an environment that is conducive to and supportive of change (Ward et al., 2004). Cognitive factors such as self-serving attitudes, attributions of blame and hostile beliefs are likely to hinder treatment readiness (Chambers et al., 2008). Theorists posit that such cognitions promote the underlying assumption that one has a right to behave in criminal ways, irrespective of the consequences (Chambers et al., 2008). Nevertheless, the possible relationships between such attitudes and treatment readiness have not yet been validated empirically. Further, childhood experiences may have a lasting and enduring impact on cognitions later in adulthood. For instance, Gibb (2002) highlighted a significant association between childhood emotional maltreatment and adult cognitive functioning. Research has neglected to explore whether childhood experiences can effect treatment readiness and cognitive functioning among adult offenders resident in a therapeutic community. AIMS & RATIONALE This study attempted to extend the present literature base by exploring the cognitive aspects of treatment readiness and determining the relationship between cognitions and treatment readiness within a therapeutic community, in accordance with the MORM model. Attributions of blame, levels and directions of hostility, and criminal thinking styles were used as indices of the cognitive aspects of treatment readiness. Attitudes, beliefs and thinking styles were explored because therapeutic communities have relatively high attrition rates and many residents fail to complete the essential period of treatment (Shine, 2007). Such cognitive factors may in turn be the target of (pre-) treatment interventions to develop and maintain engagement in order to improve the overall quality of life of offenders and reduce recidivism (McMurran et al., 2007). Further, a high proportion of residents at Grendon had adverse childhood experiences. This research aimed to explore whether negative childhood experiences have an enduring impact on the underlying cognitive functioning of offenders deemed treatment ready within a therapeutic environment. • METHOD • Participants: 73 adult men received into the therapeutic community between 2010 and 2012. 2.7% of the participants were determinate prisoners and 97.3% were prisoners serving life sentences. 43 participants were serving sentences for homicide offences, 12 participants for sexual offences, and 18 participants for violent offences. All the participants remained resident at the establishment during the time of data collection. • Measures: Treatment readiness was identified using the Corrections Victoria Treatment Readiness Questionnaire (CVTRQ), a standard assessment measure administered within the battery of psychometrics on the assessment unit which contains 20 items that assess readiness to participate in rehabilitation interventions (Casey et al., 2007). A number of psychometric measures were used to measure cognitive functioning which included the Psychological Inventory of Criminal Thinking Styles (PICTS; Walters, 1995), Blame Attribution Questionnaire (BAI; Gudjonsson & Singh, 1989), and Hostility and Direction of Hostility Questionnaire (HDHQ; Caine, Foulds & Hope, 1967). • Procedure: Ethical approval for the current study was obtained from the relevant ethical committees. The database at the prison establishment was utilised to identify residents who qualified for participation. It was ensured that the participants had completed the psychometric measures as part of a routine battery of psychometric tests upon arrival into the establishment. Participants who scored lower than the recommended cut-off of 72 on the CVTRQ were removed from the sample. The scores on the CVTRQ, BAI, PICTS, and HDHQ were collated for each of the participants. The background profiles and offending histories were recorded. • RESULTS • Reliability analyses revealed that a number of the subscales had low Cronbach’s alpha values and subsequently they were removed from further analyses. • Correlation analyses were initially used to explore the relationship between treatment readiness and criminal thinking styles. Significant negative correlations were found between the CVTRQ and; • PICTS: Mollification (rs = -.34, p < .01) • PICTS: Cut off (r = -.34, p < .01) • PICTS: Discontinuity (r = -.34, p < .01) • BAI: Mental (r = -.25, p < .05) • HDHQ: Intropunitive (rs = -.24, p < .05) • HDHQ: Extrapunitive (rs = -.37, p = .001) • HDHQ: Acting out (r = -.33, p < .01) • HDHQ: Criticism of others (r = -.27, p < .05) • A series of univariate analyses were performed in order to explore differences between participants who had witnessed domestic violence during childhood and those who had not, across each of the scales of the PICTS, BAI, HDHQ and CVTRQ. The analyses indicated that negative childhood experiences have an effect on cognitive functioning as an adult. For instance, witnesses of domestic violence during childhood scored significantly higher on the HDHQ ‘Criticism of Others’ scale as an adult in comparison to those who did not witness such domestic violence during childhood (t(71) = -2.23, p < .05). Individuals who had been victimised during childhood scored significantly higher on the PICTS ‘Discontinuity’ (U = 832.5, p < .05) and BAI ‘Guilt’ (U = 824.5, p = .05) scales compared to those who had not been victimised. DISCUSSION A relationship between treatment readiness and criminal thinking styles is indicated; as treatment readiness increases, the tendency to justify and rationalise norm-violating behaviour decreases. These findings support the hypotheses of previous researchers who suggested that attitudes such as the justification of crimes are incompatible with treatment readiness (Chambers et al., 2008). Additionally, the findings revealed that participants who attempt to eliminate fear or other psychological deterrents to criminal behaviour and have difficulty following through on initially good intentions are unlikely to be treatment ready. In support of previous theorists (e.g. Ward et al., 2004), the findings revealed that a tendency to attribute blame and responsibility for negative events on mental illness or weak self-control is incompatible with treatment readiness. A relationship between treatment readiness and levels/direction of hostility was also noted; as treatment readiness increased, the likelihood of suffering from psychological distress or self-criticism diminished. The present research revealed that individuals classified as treatment ready do not direct their hostility inwards nor do they direct their hostility outwards, onto surrounding others. In line with previous research (e.g. Gibb, 2002; Wenninger & Ehlers, 1998), the findings revealed that childhood experiences of sexual or physical abuse victimisation, or being witness to domestic violence, were related to higher levels of cognitive discontinuity, extrapunitive hostility and criticism of others during adulthood. Individuals who witnessed domestic violence during childhood were more likely to direct their hostility outwards and criticise others as an adult compared to those who had not witnessed such familial violence. Second, individuals who had experienced sexual or physical abuse and victimisation during childhood were more likely to have difficulty following through on initially good intentions because of inadequate self-discipline, compared to those who had not been victimised. Such findings are important as higher levels of cognitive discontinuity, extrapunitive hostility and criticism of others during adulthood may impede with treatment readiness, and subsequently the aims and outcomes of psychological therapy. Consequently, individuals who were either victimised during childhood or witnessed familial domestic violence, may require a pre-treatment programme in order to maximise their treatment readiness. IMPLICATIONS Theoretical Implications Treatment readiness correlates highly with criminal thinking styles, attributions of blame and hostile attitudes. Applied Implications The underlying cognitions associated with treatment readiness may be used as targets of a pre-treatment programme in order to maximise treatment readiness. The design, implementation and evaluation of pre-treatment preparation procedures for male offenders within a therapeutic community should adhere to criminal thinking styles, attribution of blame, and hostility attitudes in order to promote readiness, engagement and completion. Further, it is important for staff to be aware of the role of adverse childhood experiences in adult cognitive functioning and to consider this in the formulation of treatment needs. Please contact Harriet Kilbane for full references, a copy of the poster and further information on the full review and future research is available on request: Harriet.Kilbane@hmps.gsi.gov.uk Tel: 01296445241