Download

1 / 32
320 likes | 515 Views
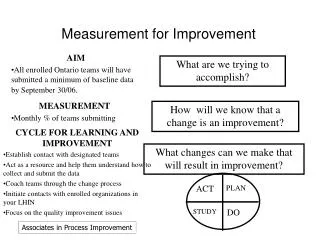
Measurement for Spread. Western Node Spread Call #3 Feb 19th, 2009. Discussion Topics for this Session. Understand what you need to measure for spread 4 categories of measurement Team examples Identifying some sampling strategies Integrating measurement into systems

E N D
Measurement for Spread Western Node Spread Call #3 Feb 19th, 2009
Discussion Topics for this Session • Understand what you need to measure for spread • 4 categories of measurement • Team examples • Identifying some sampling strategies • Integrating measurement into systems • Understand how to develop feedback loops for continuous improvement/learning
Measurement and Feedback Knowledge Management A Framework for Spread Leadership -Topic is a key strategic initiative -Goals and incentives aligned -Executive sponsor assigned -Day-to-day managers identified Social System -Key messengers -Communities -Technical support -Transition issues Set-up -Target population -Adopter audiences -Successful sites -Key partners -Initial spread strategy Better Ideas -Develop the case -Describe the ideas Communication Strategies (awareness & technical) Nolan K, Schall M, Erb F, Nolan T. Using a framework for spread: The case of patient access in the Veterans Health Administration. Joint Commission Journal on Quality and Patient Safety. 2005 Jun:31 (6):339-347.
Developing a Plan for Spread • Develop a Spread AIM • Leadership • Set-up/ infrastructure • Communication • Social System • Measurement and Feedback
Develop a Spread AIM Forms part of your measurement
Developing a Spread Aim • Spread What: • Target Level of Performance: • Spread to Whom: • Time frame:
Sample Spread Aim: Prevent Surgical Site Infections by Implementing the SSI Bundle • Spread What: All measures in the SSI Bundle • Target Level of Performance: Zero Cases of SSI • Spread to Whom: All surgical populations in our 10 hospital system • Time Frame: By September 2010
Levels of Spread Activities – Level 1 • Set-up/Infrastructure • Establishing steering committees • Orienting leadership groups • Organizing data collection • Developing materials • Identifying successful sites • General Communication • Wide spread dissemination of information about the initiative • Sending out comparative data • Holding meetings with a broad range of potential adopters
Develop a Family of Measures 4 Categories to reflect AIM and 4 levels of spread activity
Awareness of the change • Reflects spread of communication • Adoption of the Change • Reflects the integrity of the adoption • Outcome of the Change • Reflects the evidence of better ideas • Progress of the Change • Reflects the places and stage of the adoption Adoption Awareness Outcome Progress Develop Measures in 4 Categories For the Big picture on Spread
Regina Qu’Appelle Health Region Spread Measures for Med Rec • ‘Awareness of the Proposed Change’ • Number of nurses, unit clerks, pharmacists and physicians attending the group education sessions, individual mentoring sessions • ‘Adoption of the Proposed Change’ • Percentage of charts stamped by the Unit Clerk • Percentage of PIP forms used by Nurse to record BPMH • Percentage of PIP forms used by Physicians to order/address home medications • ‘Outcome of the Change’ • Percentage of identified discrepancies that are resolved by the physicians use of the PIP form • ‘Progress of the Change’ • Percentage of units and rural acute care sites reporting on the above adoption and outcome measures each week
Tracking the Adoption of the Change HMIO = Home medication and initial orders
Measures using Small Multiples: Overall System and 4 sites Overall Outcome Measure
Develop a Collection Strategy Sampling
3 Types Sampling • Simple Random Sample • Selection of data by use of random numbers generated by a random number list or mechanical devise • Systematic Random Sample • Selection of data by choosing a random starting point and then selecting data at specified intervals • Judgment Sampling • Select samples based on judgment of those with process knowledge to learn about impact of change on specific portions of a process Lloyd Provost, API & Sandy Murray CTC, The Data Guide, Learning from Data to improve Health Care, pg 2-16, 2-17.
Sampling – Just Enough • 10-15% monthly volume sufficient for QI • Minimum of 10 • Collect same way over time • Retrospective – data must be in formal charting • Prospective – data collection sheets, interviews EG. You are currently collecting discrepancy rates for MED REC monthly on admissions and you get 30 admissions per month to that unit. 30x15%=5 which is less than min, thus you would collect on min of 10 charts monthly
How do you transition from pilot to many? • Consider the # admissions to all units working on MED REC as the denominator • Thus 10-15% of the total admissions is the number of charts to review per month. Divide that by the number of units and you will get the number of charts per unit EG. You are spreading to 5 additional units. You need to still collect on the pilot unit. Each unit gets 30 admissions/month. 30x6=180 x15% = 27 charts/6 units =5 charts per unit per month. Simple random sampling: Generate a list per unit, roll dice and select chart number as per dice roll up to 5 charts per unit Systematic random sampling: Generate a list of all admissions per unit (30, 30, 30). On each list roll a dice for start number, then every 6th chart(30admissions /5charts required = every 6th chart for total of 5 charts. Repeat for each unit.
Sampling • Balance enough data with realistic workload • Ensure the data collection sheet identifies what unit/area • Sampling would most often apply to adoption measures & outcome measures • Data collection is for answering your questions about a process. Be clear on what you want to know
Ensure Accountability through a Reporting Structure Formalize regular reporting process to leader tasked with accountability for this work
Set up a regular reporting process and format • Use existing committees, structures if applicable • A senior leader needs to hold the accountability for this work • Have a system where if decline is evident in the measure, it is someone’s role to support the spread work. Brandon Regional Health MB Who Needs to Know? Who’s accountable ?
Project TITLE QIC School Participant Name, Participant Sponsor, Project Sponsor Charter Lessons Learned/Anecdotes Graphs of Measures Aim: (Aim includes your numeric goals) Make fonts large, title, labels, dates and notes very simple on graphs prior to shrinking graphs. Should be able to fit 6-8readable graphs here. If no graph yet for Measure either create “empty” graph or list Name of measure(s) not yet graphed. • Type here Why is this important?: Senior Role/Recommendations / Next Steps • Type here: what do you need from Project Sponsor, Participant Sponsor at this time to move project? • Recommendations • Next Steps for project Changes – Proposed (P), Tested (T), Implemented (I) • Type here: be clear about what is proposed (P) (to be tested) vs. testing (T), vs.implemented (I) Team Members Names/Role here QIC School Participant Contact Info: Add e-mail/phone here
Regularly Review Data and Respond Refining the spread plan and continually learning
“When the music changes, so does the dance.” African Proverb
Highlights • Measurement is meant to answer questions about how spread is going • Collect just enough to balance knowing and workload • Initial spread plan is less than 20 % of your time, 80% is refining, adjusting and supporting the changes • Be flexible, spread is a learning event not a dictatorial one!
Acknowledgements • New Generation of Ideas on Spread, Dec 8, 2008 Joe McCannon, Marie Schall, Lynn Maher, Rashad Moussad, IHI National Forum • Strategies for Spreading Improvements in Health Care, October 14, 2004Marie W. Schall, Institute for Healthcare Improvement • Holding the Gains and Spread, July 11, 2006 Bruce Harries, Improvement Associates • The Seven ‘Spreadly’ Sins, October 18, 2006 Roger Resar, MD & Carol Haraden, PhD IHI • Sustainability and Spread, August 28, 2006 Diane Jacobsen, MPH, CPHQ, IHI National Director • Continuing the Conversation Holding the Gains and Spreading Good Ideas: From Local Improvement to System-wide Change October 4, 2007 Marie Schall, MA Institute for Healthcare Improvement
References National Health Services (NHS) Modernization Agency Improvement - Sustainability and its relationship with spread and adoption. www.institute.nhs.uk/improvementleadersguides Hinchey Judge KA. Et al., Factors Contributing to Sustaining and Spreading learning Collaborative Improvements, Qualitative Research Study Findings by the Primary Care Development Corporation, Dec 2007. Nolan K, Schall M, Erb F, Nolan T. Using a framework for spread: The case of patient access in the Veterans Health Administration. Joint Commission Journal on Quality and Patient Safety. 2005 Jun:31 (6):339-347. Paul Plsek, Spreading Good Ideas for Better Health Care - A Practical Toolkit Volume 2 - Veterans Health Administration 2000 Research Series. VHA, 2000. Paul E. Plsek, Charles M. Kilo From resistance to attraction: a different approach to change - Positively Influencing Physicians Physician Executive, Nov-Dec, 1999. Dr. Lynne Maher, Emerging themes for improvement and innovation, presentation QHN Fall Forum, November 21, 2007. Developing your initial spread plan, IHI Boston Spread Workshop Feb. 2007 Barb Saunders, Spread of Improvement Efforts – Guideline for Fraser Health, March 10, 2005
References • Nolan K, Schall M, Erb F, Nolan T.; Using a framework for spread: The case of patient access in the Veterans Health Administration. Joint Commission Journal on Quality and Patient Safety. 2005 Jun;31(6):339-347 • Attewell, P. Technology Diffusion and Organizational Learning, Organizational Science, February, 1992 • Bandura A. Social Foundations of Thought and Action. Englewood Cliffs, N.J.: Prentice Hall, Inc. 1986. • Brown J., Duguid P. The Social Life of Information. Boston: Harvard Business School Press, 2000. • Cool et al. Diffusion of Information Within Organizations: Electronic Switching in the Bell System, 1971 –1982, Organization Science, Vol.8, No. 5, September - October 1997. • Dixon, N. Common Knowledge. Boston: Harvard Business School Press, 2000. • Fraser S. Spreading good practice; how to prepare the ground, Health Management, June 2000. • Gladwell, M. The Tipping Point. Boston: Little, Brown and Company, 2000. • Kreitner, R. and Kinicki, A. Organizational Behavior (2nd ed.) Homewood, Il:Irwin ,1978.
References • Langley J, Nolan K, Nolan T, Norman, C, Provost L. The Improvement Guide. San Francisco: Jossey-Bass 1996. • Lomas J, Enkin M, Anderson G. Opinion Leaders vs Audit and Feedback to Implement Practice Guidelines. JAMA, Vol. 265(17); May 1, 1991, pg. 2202-2207. • Myers, D.G. Social Psychology (3rd ed.) New York: McGraw-Hill, 1990. • Prochaska J., Norcross J., Diclemente C. In Search of How People Change, American Psychologist, September, 1992. • Rogers E. Diffusion of Innovations. New York: The Free Press, 1995. • Wenger E. Communities of Practice. Cambridge, UK: Cambridge University Press, 1998.