Download
1 / 57
570 likes | 751 Views
Endocarditis & Endovascular Infections. Thomas Hawn, July 2011. Vegetation. Tricuspid valve. Medic.med.uth.tmc.edu. Case 1. 45 yo female S/P MVA ARDS in the ICU x 15 d with new onset fever. PE IJ central line along with 2 peripheral ivs. Question:

E N D
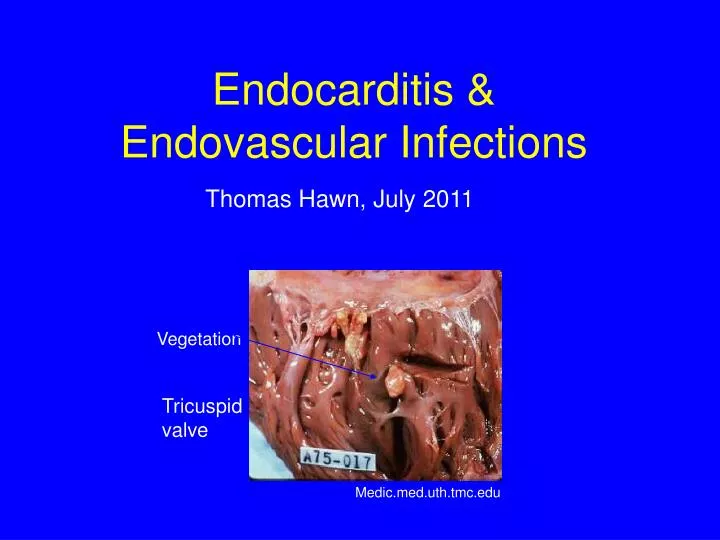
Endocarditis & Endovascular Infections Thomas Hawn, July 2011 Vegetation Tricuspid valve Medic.med.uth.tmc.edu
Case 1 45 yo female S/P MVA ARDS in the ICU x 15 d with new onset fever. PE IJ central line along with 2 peripheral ivs. Question: How do you diagnose a CVC infection?
Central Venous Catheter Infections Diagnostic Recommendations If CVC infection is suspected, 1. Draw 2 sets of bld cxs (one percutaneously) 2. Check paired quantitative or qualitative with time to positivity monitoring 3. If catheter is removed, send tip for culture. Criteria for positivity: >15 CFU by semi-quantitative method (roll-plate) >100 CFU by quantitative method (sonication)
Central Venous Catheter Infections Case: Blood culture grow Staphylococcus aureus in 2 out of 2 sets (4 bottles). Catheter 100 CFU/ml + in 14h Vein 15 CFU/ml + in 18h Question: What is your management recommendation? Should the line be removed? Duration of Rx? Should a TTE or TEE be obtained?
Central Venous Catheter Infections Criteria for positivity Paired quantitative: catheter:vein cfu ratio >3 Unpaired quantitative: catheter cx >100 cfu/ml Differential time: >120 minutes SensSpec Paired quantitative 79 94 Siegman-Igra, meta-analysis (cath:vein ratio>3-10:1) Unpaired quantitative 78 96 Siegman-Igra, meta-analysis (CFU/ml>15-100) Differential time to positivity 89 100 Gaur et al, n=33 (time>120 minutes) 96 100 Blot et al (1998), n=64, (time > 120 minutes) 94 91 Blot et al (1999), n=28, (time > 120 minutes)
Uncomplicated CVC Bacteremia 1) No septic emboli 2) Negative surveillance cultures 2-4 d after starting therapy 3) Removable focus of infection 4) Not immunocompromised 5) Rapid clinical resolutions of sxs within 72h of starting abx and removing focus of infection 6) No indwelling prosthetic devices or underlying heart disease
Should the line be removed in S. aureus bacteremia? S. aureusbacteremia, n=244 Management recommended: remove focus of infection, check surveillance cultures, TEE, start therapy (decide duration based on whether endocarditis present) Cure rate: Recommendations followed: 79.5% Recommendations not followed: 64.4% Foreign body removed: 83.7% Foreign body not removed: 43.5% Fowler et al (1998) CID 27: 478-86
Case 2 50 yo F in ICU with fever Bld Culture: Tunneled line: +Candida in 2/2 bottles Peripheral: No growth Questions 1. Can you treat through the line? 2. What anti-fungal treatment do you start? 3. When do you change Rx after species known? 4. When do you get MICs for fluconazole?
IDSA Candida 2009 Guidelines Pappas et al (2009) CID 48: 503-35 Candidemia in non-neutropenic host Initial Rx: Fluconazole 800 mg load, then 400 mg qday OR Echinocandinqday (A-I) Echinocandin preferred if higher illness severity or recent azole exposure (A-III) Remove catheter (A-II) Search for metastatic foci Rx duration: 2 wks if uncomplicated (A-III)
Micafungin versus Caspofungin for Treatment of Candidemia and Other Forms of Invasive Candidiasis Pappas et al (2007) CID 45: 883-93 Rx Success associated with Catheter Removal RDBPCT, n=595 candidemic pts Treatment Success Catheter removed 77.9% Catheter not removed 63.2% P=0.001 But, also some controversial & contradictory data: Nucci et al CID 51: 295-303 (2010), Horn et al Eur J Clin Micro Infection 29: 223-29 (2010), Kuse et al Lancet 369: 1519-1527 (2007)
Rebolietal (2007) NEJM 356: 2472 Anidulafungin non-inferior to fluconazole, But, … possibly more efficacious
IDSA Candida 2009 Guidelines Drug choice & need to check sensitivities C. albicans: sensis not routine, based on risks C. glabrata: echinocandin preferred (B-III) or check flucsensi C. krusei: no fluc C. parapsilosis: fluc preferred (B-III)
Short Term CVC Management Mermel et al CID 2009 IDSA Catheter Rx Recs
Long Term CVC Management Mermel et al CID 2009 IDSA Catheter Rx Recs
Case 3 40 yo M with mitral valve prolapse. Dentist plans to place orthodontic brackets. 50 yo F with a history of endocarditis will undergo cystoscopy What do you recommend for IE prophylaxis?
What is the highest risk of bacteremia exposure? Cumulative exposure measures CFU per minute per ml per year of bacteria Tooth extraction Dental Exam Mucoperiosteal surgery Daily life Flossing Brushing teeth Chewing NT tube Risk (Relative to tooth extraction) 1 222 5,555 1,693,556 365,000 702,556 136,778 166 2007 guidelines: Emphasize that daily activities incur highest risk, rather than procedures.
What are risk factors for IE? IE incidence #/100,000 person years General population 4.9 Prior endocarditis Rheumatic heart disease Congenital heart disease: overall VSD with medical Rx VSD with surgical Rx Aortic stenosis Pulmonic stenosis Prosthetic valve MVP with murmur MVP without murmer Steckelberg & Wilson 1999 740 440 120 220 60 180 20 308-383 52 4.6
2007 AHA Guidelines • Cardiac Conditions with recommended prophylaxis: • 1. Prosthetic cardiac valve • 2. Previous IE • 3. Congenital Heart Disease: • A. Unrepaired cyanotic CHD, including palliative shunts & conduits • B. Completely repaired CHD with prosthetic material or device, during the first 6 months after the procedure • C. Repaired CHD with residual defects at the site or adjacent to the site of a prosthetic patch or device • 4. Cardiac transplant recipients who develop cardiac valvulopathy • Compared to 1997: Simplified list with emphasis on risk of adverse outcome from IE rather than risk of acquisition. • (no longer recommended for MVP or RHD)
2007 AHA Guidelines Procedures for which endocarditis is recommended for the above categories of patients: 1. All dental procedures that involve manipulation of gingival tissue or the periapical region of teeth or perforation of the oral mucosa. 2. Respiratory tract or infected skin/soft tissue procedures 3. NOT recommended for GU or GI procedures solely to prevent IE Compared to 1997: Simplified list of which procedures qualify (no GU/GI, criteria for dental procedure straightforward)
Cases 4 & 5 HPI: 14 yo M 2 m h/o of fever, HA, myalgias. RLQ pain led to appendectomy w/ necrotizing lymphadenitis. Left calf pain resolved with Abx. After Abx, fever returned Then, R wrist swollen & tender R thigh pain developed. PE: T 39.3, P 108, BP 128/35 II/VI systolic murmur splinter hemorrhages in 3 nails petechial rash on legs Labs: Bld Cx 6/6 bottles Viridans strep 45 yo M h/o ESLD, HCV, EtOH Fever x 3d. Also with SOB and abdominal pain. PE: Tm 38.5 Gingivitis CV III/VI SEM over LUSB, ?splinter hemorrhages 2 nails Labs: Bld Cx: 1/6 bottles with Viridans strep
Questions: • What is your DDx? • How many modified Duke criteria does this patient have? • How useful are the modified Duke criteria? • What work-up is needed?
DDx of Endocarditis A. associated with neoplasms: atrial myxoma, marantic (adenoCa), carcinoid B. associated with autoimmune: rheumatic heart disease, SLE (Libman-Sacks endocarditis), anti-phospholipid syndrome, polyarteritis nodosa, Behcet’s disease C. Postvalvular operation: thrombus, sutures D. Other: eosinophilic heart disease, ruptured mitral chordae, myxomatous degeneration
Modified Duke Clinical Criteria • Definite IE • Pathological criteria: • Microorganisms: demonstrated by culture or histology in a vegetation, in a vegetation that has embolized, or in an intracardiac abscess, or • Pathologic lesions: vegetation or intracardiac abscess present, confirmed by histology showing active endocarditis. • Clinical criteria • 2 major criteria, or • 1 major and 3 minor criteria • 5 minor criteria
Modified Duke Clinical Criteria Possible IE 1 major and 1 minor 3 minor Rejected Firm alternate diagnosis for manifestations of endocarditis Resolution of manifestations of endocarditis with antibiotic therapy for ≤ 4 days, or No pathological evidence of IE at surgery or autopsy, after antibiotic therapy for ≤ 4 days.
Major Criteria 1. Positive blood culture for IE A. Typical microorganism consistent with IE from 2 separate blood cultures as noted below: viridans streptococci, Streptococcus bovis, HACEK group, Staphylococcus aureus, or community-acquired enterococci, in the absence of a primary focus B. Microorganisms consistent with IE from persistently positive blood cultures as defined as (i) ≥2 positive cultures of blood samples drawn >12 hours apart (ii) all of 3 or a majority of ≥4 separate cultures of blood (with the first and last samples drawn ≥1 hour apart) iii. Coxiella: + Bld cx or anti-phase I Ab titer>1:800
Bacteremia & IE Likelihood PathogenIE:non IE Ratio S. mutans S. bovis S. sanguis S. mitior E. faecalis S. anginosus Grp G Streptococcus Grp B Streptococcus Grp A Streptococcus 14.2 : 1 5.9 : 1 3.0 : 1 1.8 : 1 1.0 : 1.2 1.0 : 2.6 1.0 : 2.9 1.0 : 7.4 1.0 : 32.0
Major Criteria 2. Evidence of endocardial involvement A. Positive echocardiogram for IE defined as (i) oscillating intracardiac mass on valve or supporting structures, in the path of regurgitant jets, or on implanted material in the absence of an alternative anatomic explanation, or (ii) abscess, or (iii) new partial dehiscence of prosthetic valve, or B. New valvular regurgitation (worsening or changing or pre-existing murmur not sufficient)
Minor Criteria 1. Predisposition: predisposing heart condition or intravenous drug use 2. Fever: temperature ≥ 38.0 C 3. Vascular phenomena: major arterial emboli, septic pulmonary infarcts, mycotic aneurysm, intracranial hemorrhage, conjunctival hemorrhage, and Janeway lesions 4. Immunologic phenomena: glomerulonephritis, Osler’s nodes, Roth spots, and rheumatoid factor 5. Microbiological evidence: positive blood culture but does not meet a major criteria as noted above or serologic evidence of active infection with organism consistent with IE (excludes single positive cultures for coagulase-negative Staphylococci and organisms that do not cause endocarditis).
Clinical Manifestations Osler’s nodes Splinter hemorrhages Janeway’s lesions Conjunctival hemorrhages Mylonakis, NEJM, 2001
Clinical Manifestations Septic pulmonary emboli www.vh.org
Case 6Pt w/ endocarditis w/u has 1 major & 1 minor Duke’s Criteria • How hard do you search for more criteria? • When do you recommend a brain MRI? • When do you recommend a TEE? • Should all pts with CVC-associated S. aureusbacteremia get a TEE?
Role of Transesophageal ECHO in diagnosing IE 1. Prosthetic valves 2. Suspected complication (such as perivalvular abscess) 3. Those in “Possible Endocarditis” category 4. ? Negative TTE & S. aureus bacteremia
Should all patients with S. aureus bacteremia have a TEE? Arguing in favor: 1) Increased sensitivity leads to more diagnoses & better Rx TTE sensitivity=32% TEE sensitivity=100% 2) ? Cost effective (save costs of lengthy treatment) Arguing against: 3) TEE more labour intensive 4) Small vegetations may be adequately treated with short course treatment.
Clinical Manifestations: Complications Mycotic aneurysm www.pharmacology2000.com
Duval et al Ann Int Med 152: 497 (2010) High rate of lesions in neurologically asymptomatic cases
Assessment of Duke Criteria • Sensitivity: 80% for definite IE • 100% for definite + possible IE • Negative predictive value >98% for rejected category • Adopted modifications from Li et al (2000) • a. S. aureus bacteremia should be a major criteria regardless of the source (community or nosocomial) • b. Eliminate the ECHO minor criteria since TEE’s are more widely used now • c. Add Coxiella to list of major criteria (a single positive blood culture or antiphase I IgG antibody titer > 1:800). • d. To increase specificity, change the category “possible IE” to cases with 1 major and 1 minor criteria or 3 minor criteria.
Case 7 30 yo M with h/o IDU with fever Diagnosed with MV IE 2° MRSA Started on vancomycin/gentamicin Daily cultures positive x 8 d Questions: Should a vancomycin MIC be obtained? Should vancomycin troughs be obtained? Should a different drug be used? Does this patient need cardiac surgery?
Randomized trial Inclusion: positive SA blood cx Randomize to: daptomcyin (n=124) vs. standard therapy ( b-lactam or vancomycin/gentamicin 1 mg/kg x 4d) Results: Overall success ITT: daptomycin 42.7% standard Rx: 39.3% Conclusion: Daptomycin is non-inferior to standard Rx Median duration of bacteremia: Dapto Std Rx P MRSA 8d 9d 0.28 MSSA 4d 3d 0.25 Fowler et al NEJM 2006
Vancomycin Dose & MICs IDSA Guideline for complicated MRSA infection: Goal vanc trough is 15-20 ucg/ml (Rybak et al CID 2009) Target AUC/MIC Ratios Difficult to achieve with MRSA Monte Carlo Simulations of Different Dosing (Patel et al CID 2011) Trough of 15-20 Trough of 10-15 Are high MICs associated with poor outcomes? YES Prospective observational study (Soriano et al CID 2008) Inclusion: MRSA bacteremia, n=414 If vancomycin MIC = 2 OR for mortality: 6.39 (1.68-24.3)
Do high vanc troughs help? YES Kullar et al CID 2011 Retrospective study, n=320 MRSA bacteremia NO Hidayatet al Arch Int Med 2008 Prospective cohort study Inclusion: MRSA sputum, blood, wound Measure vancomycin MIC Compare high (≥2) vs low (<2) MIC Compare achievement of trough goal target of 15 ucg/ml
Is Anything Better than VancFor MRSA? Unknown Cidalvs PK/PD Adverse Static Effects Vancomycin C +/- Problem Renal Daptomycin C Not for lung Myopathy Linezolid S OK BM Ceftaroline C OK OK TMP-SMX C OK Renal, BM
Case 8: Rx ?s 3. 65 yo female with 4 weeks of fever, myalgias, nausea and decreased appetitie. ECHO: MV vegetation with severe MR. 4. 30 year old male with h/o IVDU and dental caries with fever for 1 day after recent injection. ECHO: AV vegetation with severe AI. Question: What empiric treatment do you recommend before the results of blood cultures are known? What antibiotics do you recommend for viridans strep? Who can be treated for 2 wks?
Empiric Antibiotic Selection Empiric Therapy for IE Main goal is to treat acute IE, most often caused by S. aureus Acute IE: Vancomycin +/- gentamicin Subacute IE: more difficult and less important to Rx empirically. Vancomycin + ceftriaxone covers many of the important organisms.
AHA: Rx of Viridans Strep IE Viridans streptococci & S. bovis, PCN susceptible (MIC ≤0.12 mg/ml) i. PCN G 12-18 mU iv/day x 4 wks, ii. ceftriaxone 2g iv or im qd x 4 wks, iii. PCN G 12-18 mU iv qd + x 2 wks, gentamicin 1 mg/kg iv q8h iv. vancomycin 1g iv bid x 4 wks (for b-lactam allergic pts)
AHA: Rx of Viridans Strep IE • Viridans streptococci & S. bovis, • relatively resistant to PCN (MIC > 0.12 mg/ml & < 0.5 mg/ml) • i. PCN G 24 mU iv/day x 4 wks • + gentamicin 3 mg/kg iv qd x 2 wks • Ceftriaxone 2g iv qd x 4 wks • + gentamicin 3 mg/kg iv qd x 2 wks • iii. vancomycin 1g iv bid x 4 wks (for b-lactam allergic pts)
AHA: Rx of Enterococcus, Abiotrophia, & Grunulicatella IE i. PCN G 18-30 mU iv/day x 4-6 wks + gentamicin 1 mg/kg iv q8h x 4-6 wks ii. ampicillin 12 g/day iv x 4-6 wks + gentamicin 1 mg/kg iv q8h x 4-6 wks iii. vancomycin 1g iv bid x 6 wks + gentamicin 1 mg/kg iv q8h x 6 wks (for b-lactam allergic pts)
AHA: Rx of HACEK IE i. ceftriaxone 2g iv/im qd x 4 wks (or other 3rd or 4th gen. cephalosporin) ii. Ampicillin-sulbactam 12g iv/day x 4 wks iii. Ciprofloxacin 500 mg po bid or 400 mg iv bid x 4 wks (less experience with quinolones & HACEK)
Case 9 16 yo male with a 1 week history of fever to 103 F. Developed confusion, blurrred vision and abdominal pain. Head CT showed hypodense lesions bilaterally in the parietal lobe, abdominal CT showed a 2 cm splenic infarct, and an ophthalmologic exam showed bilateral emboli. 4 out of 4 cultures grew MRSA. ECHO showed mild MR and a vegetation on the anterior leaflet. Does this patient need cardiac surgery?