Download
1 / 1
10 likes | 102 Views
Methods. Introduction. Conclusion. References. Results. Results. Results. Under Diagnosis of Floppy Eyelid Syndrome in Patients with Obstructive Sleep Apnea Charles Bouchard MD, Sarah Maki, Bruce Gaynes OD PharmD , Ron Price, Dan Valdez, Nidhi Undevia MD

E N D
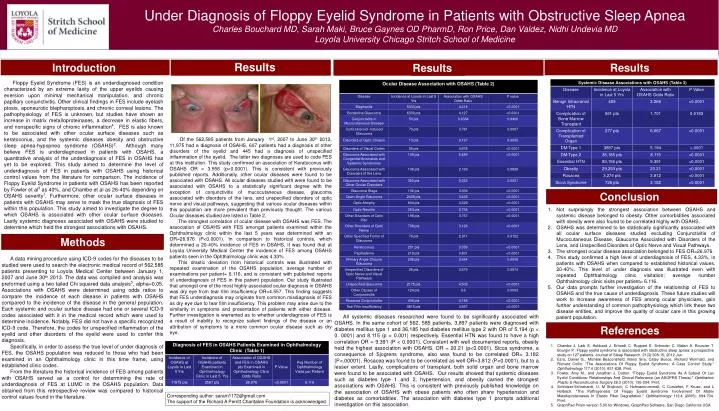
Methods Introduction Conclusion References Results Results Results Under Diagnosis of Floppy Eyelid Syndrome in Patients with Obstructive Sleep Apnea Charles Bouchard MD, Sarah Maki, Bruce Gaynes OD PharmD, Ron Price, Dan Valdez, NidhiUndevia MD Loyola University Chicago Stritch School of Medicine Floppy Eyelid Syndrome (FES) is an underdiagnosed condition characterized by an extreme laxity of the upper eyelids causing eversion upon minimal mechanical manipulation, and chronic papillary conjunctivitis. Other clinical findings in FES include eyelash ptosis, aponeuroticblepharoptosis,and chronic corneal lesions. The pathophysiology of FES is unknown, but studies have shown an increase in matrix metalloproteinases, a decrease in elastic fibers, and nonspecific signs of chronic inflammation4. FES is also known to be associated with other ocular surface diseases such as keratoconus, and the systemic diseases obesity and obstructive sleep apnea-hypopnea syndrome (OSAHS)2. Although many believe FES is underdiagnosed in patients with OSAHS, a quantitative analysis of the underdiagnosis of FES in OSAHS has yet to be explored. This study aimed to determine the level of underdiagnosis of FES in patients with OSAHS using historical control values from the literature for comparison. The incidence of Floppy Eyelid Syndrome in patients with OSAHS has been reported by Fowler et al3 as 40%, and Chambe et al as 26-40% depending on OSAHS severity1. Furthermore, other ocular surface diseases in patients with OSAHS may serve to mask the true diagnosis of FES within this population. This study aimed to investigate the degree to which OSAHS is associated with other ocular surface diseases. Lastly systemic diagnoses associated with OSAHS were studied to determine which held the strongest associations with OSAHS. Of the 562,585 patients from January 1st, 2007 to June 30th 2013, 11,975 had a diagnosis of OSAHS, 607 patients had a diagnosis of other disorders of the eyelid and 445 had a diagnosis of unspecified inflammation of the eyelid. The latter two diagnoses are used to code FES at this institution. This study confirmed an association of Keratoconus with OSAHS OR = 3.556 (p<0.0001). This is consistent with previously published reports. Additionally, other ocular diseases were found to be associated with OSAHS. All ocular diseases studied with were found to be associated with OSAHS to a statistically significant degree with the exception of conjunctivitis of mucocutaneous disease, glaucoma associated with disorders of the lens, and unspecified disorders of optic nerve and visual pathways, suggesting that various ocular diseases within this population are more prevalent than previously thought. The various Ocular diseases studied are listed in Table 2. The strongest correlation of ocular disease with OSAHS was FES. The association of OSAHS with FES amongst patients examined within the Ophthalmology clinic within the last 5 years was determined with an OR=26.976 (P<0.0001). In comparison to historical controls, which determined a 20-40% incidence of FES in OSAHS, it was found that at Loyola University Medical Center the incidence of FES among OSAHS patients seen in the Ophthalmology clinic was 4.33%. This drastic deviation from historical controls was illustrated with repeated examination of the OSAHS population, average number of examinations per patient= 6.116, and is consistent with published reports of underdiagnosis of FES in this patient population. Our study illustrated that amongst one of the most highly associated ocular diagnosis in OSAHS was dry eye from tear film insufficiency OR=4.557. This finding suggests that FES underdiagnosis may originate from common misdiagnosis of FES as dry eye due to tear film insufficiency. This problem may arise due to the similarity in symptoms and presentation of patients with either disease. Further investigation is warranted as to whether underdiagnosis of FES is a result of inability to recognize salient findings of the disease or an attribution of symptoms to a more common ocular disease such as dry eye. Not surprisingly the strongest association between OSAHS and systemic disease belonged to obesity. Other comorbidities associated with obesity were also found to be correlated highly with OSAHS. OSAHS was determined to be statistically significantly associated with all ocular surface diseases studied excluding Conjunctivitis of Mucocutaneous Disease, Glaucoma Associated with Disorders of the Lens, and Unspecified Disorders of Optic Nerve and Visual Pathways. The strongest ocular disease association belonged to FESOR=26.976. This study confirmed a high level of underdiagnosis of FES, 4.33%, in patients with OSAHS when compared to established historical values, 20-40%. This level of under diagnosis was illustrated even with repeated Ophthalmology clinic visitation; average number Ophthalmology clinic visits per patient= 6.116. Our data prompts further investigation of the relationship of FES to OSAHS and the true cause of underdiagnosis. These future studies will work to increase awareness of FES among ocular physicians, gain further understanding of common pathophysiology which link these two disease entities, and improve the quality of ocular care in this growing patient population. A data mining procedure using ICD-9 codes for the diseases to be studied were used to search the electronic medical record of 562,585 patients presenting to Loyola Medical Center between January 1, 2007 and June 30th 2013. The data was compiled and analysis was preformed using a two tailed Chi squared data analysis5, alpha=0.05. Associations with OSAHS were determined using odds ratios to compare the incidence of each disease in patients with OSAHS compared to the incidence of the disease in the general population. Each systemic and ocular surface disease had one or several ICD-9 codes associated with it in the medical record which were used to determine incidence. Notably, FES did not have a specific recognized ICD-9 code. Therefore, the codes for unspecified inflammation of the eyelid and other disorders of the eyelid were used to confer this diagnosis. Specifically, in order to assess the true level of under diagnosis of FES, the OSAHS population was reduced to those who had been examined in an Ophthalmology clinic in this time frame, using established clinic codes. From the literature the historical incidence of FES among patients with OSAHS served as a control for determining the rate of underdiagnosis of FES at LUMC in the OSAHS population. Data obtained from this retrospective review was compared to historical control values found in the literature. All systemic diseases researched were found to be significantly associated with OSAHS. In the same cohort of 562, 585 patients, 3,897 patients were diagnosed with diabetes mellitus type 1 and 36,185 had diabetes mellitus type 2 with OR of 5.194 (p < 0. 0001) and 8.115 (p < 0.001) respectively. Essential HTN was found to have a high correlation OR = 9.391 (P < 0.0001). Consistent with well documented reports, obesity held the highest association with OSAHS, OR = 20.21 (p<0.0001). Sicca syndrome, a consequence of Sjogrens syndrome, also was found to be correlated OR= 3.182 (P<.00001). Rosacea was found to be correlated as well OR=3.812 (P<0.0001), but to a lesser extent. Lastly, complications of transplant, both solid organ and bone marrow were found to be associated with OSAHS. Our results showed that systemic diseases such as diabetes type 1 and 2, hypertension, and obesity carried the strongest associations with OSAHS. This is consistent with previously published knowledge on the association of OSAHS with obese patients who often share hypertension and diabetes as comorbidities. The association with diabetes type 1 prompts additional investigation on this association. Chambe J. Laib S. Hubbard J. Erhardt C. Ruppert E. Schroder C. Malan A. Bourcier T. Bourgin P.: Floppy eyelid syndrome is associated with obstructive sleep apnea: a prospective study on 127 patients. Journal of Sleep Research. 21(3):308-15, 2012 Jun. Ezra, Daniel G., Michèle Beaconsfield, Mano Sira, CateyBunce, Richard Wormald, and Richard Collin. "The Associations Of Floppy Eyelid Syndrome: A Case Control Study." Ophthalmology 117.4 (2010): 831-838. Print. Fowler, Amy M., and Jonathan J. Dutton. "Floppy Eyelid Syndrome As A Subset Of Lax Eyelid Conditions: Relationships And Clinical Relevance (an ASOPRS Thesis)." Ophthalmic Plastic & Reconstructive Surgery 26.3 (2010): 195-204. Print. Schlotzer-Schrehardt, U, M Stojkovic, C Hofmannrummelt, C Cursiefen, F Kruse, and L Holbach. "The Pathogenesis Of Floppy Eyelid Syndrome Involvement Of Matrix Metalloproteinases In Elastic Fiber Degradation." Ophthalmology 112.4 (2005): 694-704. Print. GraphPad Prism version 5.00 for Windows, GraphPad Software, San Diego California USA Corresponding author: saram1172@gmail.com The support of the Richard A Perritt Charitable Foundation is acknowledged






