Download

1 / 96
1.02k likes | 1.25k Views
Heart Failure [HF]. Definition of HF. Heart failure is a complex clinical syndrome that can result from any structural or functional cardiac disorder that impairs the ability of the ventricle to fill with or eject blood

E N D
Definition of HF • Heart failure is a complex clinical syndrome that can result from any structural or functional cardiac disorder that impairs the ability of the ventricle to fill with or eject blood • As a consequence the heart fails to pump sufficient blood to meet the body's metabolic needs.
DD of Dyspnea [shortness of breath] • Cardiac: • Heart failure • Angina: retrosternal pain radiates to arm and jaw-pain ppt by exertion, relieved by rest • Pulmonary embolism: acute dyspnea- hemoptysis diagnosed by pulmonay angiography • Pulmonary hypertension: Ausc.: accentuated 2nd heart sound- dullness in the 2nd intercostal space • Other causes: • Respiratory disease [ bronchitis]= longer in duration- normal heart and ECG exam.+ diffuse rhonchi • Anemia = CBC • Obesity =BMI and normal chest and heart examination • History of Drug intake: -blockers in asthmatic patient- exacerbation of heart failure by -blockers, NSAIDS, Diltiazem
DD of generalized edema • Cardiac: occurs in the dependent parts of the body: ankle, sacral- bilateral pitting edema-edema of LL preceeds ascites • Renal: nephritic or nephrotic syndrome, first appears in eye lids and is associated with polyurea or oliguria-hematuria • Hepatic: edema of LL and ascites + features of liver cirrhosis: cirrhosis- splenomegaly- jaundice • Nutritional: long history of inadequate diet or diarrhea. First in LL associated with features of nutritional deficiency • Drugs: fluid retention from steroids, NSAIDs, nifedipine and amlodipine [CCBs]
Goals and guidelines of therapy • The ACC/AHA Task Force recommends that most patients with HF should be routinely managed with a combination of four types of drugs: • A Diuretic, • An ACE Inhibitor, • A -adrenergic Blocker, • And (Usually) Digitalis. • An Aldosterone Antagonist (E.G., Spironolactone) Is A Fifth Class Of Drug Recommended For Patients With Advanced HF.
Goals and guidelines of therapy • The ultimate goal is to: • prolong survival in individuals • and reduce mortality rates within the population of patients with HF. • Short of a heart transplant, none of the treatment measures are curative.
Main guidelines of therapy • medical management of HF includes: • correction of underlying disease states (e.g., hypertension, ischemic heart disease, arrhythmias, lipid disorders, anemia, or hyperthyroidism) • moderate physical activity • immunization with influenza and pneumococcal vaccines to reduce the risk of respiratory infections, and discontinuation of possible drug-induced causes. • A sodium-restricted diet and diuretics are required if fluid retention is evident. • Amiodarone is indicated in the treatment of symptomatic ventricular tachycardia and atrial fibrillation associated with HF.
MANAGEMENT OF HEART FAILURE
Physical Activity • Edema can be minimized by use of elastic stocks • During acute exacerbations, bed rest and restricted physical activity • Renal perfusion is increased in the prone position, resulting in diuresis
Sodium-Restricted Diet • In patients with hypertension or evidence of fluid retention, but is not required in all patients. • Dietary sodium can be reduced to 2 to 4 g of NaCl is more palatable and leads to better adherence than a severely salt-restricted diet.
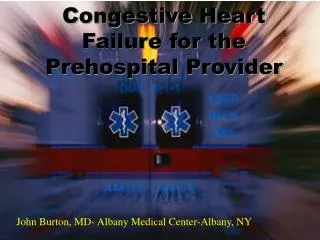
Ion movements during the contraction of cardiac muscle. ATPase = adenosine triphosphatase.
1-Diuretics in HF • are indicated in patients with circulatory congestion (pulmonary and peripheral edema) and/or cardiac distension (enlarged heart on chest radiograph). • They produce symptomatic relief more rapidly than other drugs for HF. • However, monotherapy with diuretics is discouraged, diuretics should be combined with an ACE inhibitor and a β-blocker unless contraindications exist.
1-Diuretics in HF • By enhancing renal excretion of sodium and water, diuretics diminish vascular volume, thus relieving ventricular and pulmonary congestion and decreasing peripheral edema. • If diuresis is too vigorous, intravascular volume depletion: • hypotension • paradoxical decrease in CO • Weight loss exceeding 1 kg/day is to be avoided except in patients with acute pulmonary edema.
1-Diuretics in HF • Diuresis after IV administration: • The onset of response after an IV injection of loop diuretics is 10 minutes or less, • peaking within the first 30 minutes, • and usually abating within 2 hours. • Diuresis after oral administration: • usually begins 30 to 90 minutes after the oral administration of loop diuretics • it peaks within the first or second hour • and lasts for 6 to 8 hours.
Aldosterone Antagonists (e.g., eplerenone and spironolactone) • The Randomized Aldactone Evaluation Study Investigators found that : • protective effect of spironolactone was related more to: a reduction in aldosterone-induced vascular damage and myocardial or vascular fibrosis than to its diuretic effect. • Similarly, with 25 to 50 mg of eplerenone: reduced mortality was observed in patients with left ventricular dysfunction following a recent MI • NO EVIDENCE that the direct acting potassium sparing diuretics amiloride or triamterene exert a similar protective effect.
2-Angiotensin-Converting Enzyme Inhibitors • Drugs with vasodilating properties have become a primary treatment modality of HF. • Arterial dilation provides symptomatic relief of HF by decreasing arterial impedance (afterload) to left ventricular outflow. • Venous dilation decreases left ventricular congestion (preload). • The combination of these two properties provides additive benefits to alleviate the symptoms of HF and increase exercise tolerance.
Angiotensin-Converting Enzyme Inhibitors • ACE inhibitors are not only vasodilators but they also favorably modify cardiac remodeling • they have a more tolerable side effect profile. • they slow the rate of mortality in HF more than the hydralazine-nitrate combination • These advantages, led ACC/AHA to recommend ACE inhibitors as the drugs of choice for initial therapy,
2- Angiotensin-Converting Enzyme Inhibitors • The 2001 ACC/AHA guidelines state: • “ACE inhibitors should be prescribed to all patients with HF due to left ventricular systolic dysfunction unless they have a contradiction to their use or have been shown to be unable to tolerate treatment with these drugs. • ACE inhibitors should not be prescribed without a diuretic in patients with current or recent history of fluid retention. prescribers should ensure that the appropriate doses of diuretics before and during treatment with these drugs.” • Their value in diastolic failure still is being investigated.
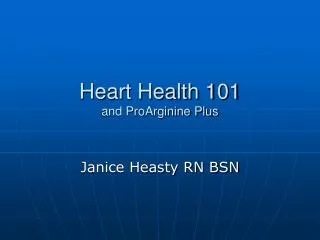
Effect of enalapril on the mortality of patients with congestive heart failure.
2- The Angiotensin Receptor Blockers [ARBs] • A related class of drugs are the angiotensin receptor inhibitors (candesartan [Atacand], eprosartan [Teveten], irbesartan [Avapro], losartan [Cozaar], olmesartan [Benicar], telmisartan [Micardis], and valsartan (Diovan). • Advantages over ACEIs • The receptor inhibitors offer theoretic advantages over ACE inhibitors by being: • more specific for angiotensin II blockade • with a lower risk of drug-induced cough.
ARBs • Mechanism of action • Block Ang II receptor type I • Advantages over ACEIs • Does not block type II angiotensin II receptors so maintain antiproliferative and VD effect • Bradykinin is converted to kinins so no dry cough Disadvantages against ACEIs • No action on type IV angiotensin II receptor thrombotic tendency • No maintainance of bradykinin no additional VD
2-The Angiotensin Receptor blockers [ARBs] • Advantages of ACEIs over ARBs • More importantly, there is evidence that ACE inhibitors have a more favorable effect on prevention of cardiac remodeling by unclear mechanisms. • Currently, ARBs are reserved for use in those who fail to tolerate ACE inhibitors (e.g., angioedema or intractable cough) or during pregnancy.
The Angiotensin Receptor blockers [ARBs] • Clinical trials on ARBs • Preliminary results of clinical trials with several of the angiotensin-receptor blockers (ARBs) have been encouraging, but more data are needed relative to their effects on restricting cardiac remodeling and reducing mortality. • There have been more clinical trials with losartan, but only valsartan has FDA approved labeling for treatment of HF.
3-β-Adrenergic Blocking Agents • Cardiac adrenergic drive initially supports the performance of the failing heart, but long-term activation of the sympathetic nervous system exerts deleterious effects that can be antagonized by the use of β-blockers. • Extended release metoprolol (Toprol XL) and carvedilol are FDA approved for use in HF.
3-β-Adrenergic Blocking Agents • While some patients can initially have a temporary worsening of symptoms, • continued use results in improved quality of life, • fewer hospitalizations, • and most importantly, longer survival. • The AHA/ACC guidelines state that β-blockers should be prescribed to all patients with stable HF due to left systolic dysfunction and with mild to moderate symptoms unless they have a contraindication to their use or have been shown to be unable to tolerate treatment with these drugs. Generally they are used in combination with diuretics and an ACE inhibitor (with or without digoxin).
Cumulative mortality in patients with heart failure treated using placebo or metoprolol
3-β-Adrenergic Blocking Agents • β-Blockers are also an important part of the treatment of patients with HF symptoms due to diastolic failure,. For these patients a nonselective β-blocker like propranolol can be a therapy of choice in selected patients by: • slowing the HR • allowing improved ventricular filling.
4-Digitalis Glycosides (Digoxin) • Mechanism of action: Digitalis glycosides binds to and inhibits sodium-potassium (Na+-K+) adenosine triphosphatase (ATPase) in cardiac cells, decreasing outward transport of sodium and increasing intracellular concentrations of calcium within the cells. Calcium binding to the sarcoplasmic reticulum causes an increase in the contractile state of the heart.
Mechanism of action of cardiac glycosides, or digitalis. ATPase = adenosine triphosphatase
4- Digitalis Glycosides (Digoxin) • Recent evidence suggests that even at serum concentrations below those associated with positive inotropism • , digoxin has beneficial autonomic effects by reducing sympathetic tone and stimulating parasympathetic (vagal) responses.
4-Digitalis Glycosides (Digoxin) • In addition to effects on contractility, digoxin decreases the conduction velocity and prolongs the refractory period of the atrioventricular (AV) node. • This AV node–blocking effect prolongs the PR interval and is the basis for use of digoxin in slowing the ventricular response rate in patients with atrial fibrillation and other supraventricular arrhythmias.
4- Digitalis Glycosides (Digoxin) • In the past few years, several studies have confirmed that digoxin should be considered to improve the symptoms and clinical status of patients with HF, in combination with diuretics, an ACE inhibitor, and a β-blocker.
4- Digitalis Glycosides (Digoxin) • Digoxin can be used early to reduce symptoms in patients who have started, but not yet responded to, treatment with an ACE inhibitor and a β-blocker. • Alternatively, treatment with digoxin can be delayeduntil the patient's response to an ACE inhibitor and β-blocker has been defined and used only for those patients who remain symptomatic despite the other drugs. • Monotherapy with digoxin or in combination with only a diuretic is no longer recommended.
4- Digitalis Glycosides (Digoxin) • Digoxin can also be considered in patients with HF who also have chronic atrial fibrillation, although β-blockers may be more effective than digoxin in controlling the ventricular response, especially during exercise. • the digitalis glycosides are not useful in diastolic HF and, in fact, may worsen this form of left ventricular dysfunction.
4- Digitalis Glycosides (Digoxin) • Most clinicians prefer to use the brand name product (Lanoxin) with a high bioavailability from other digoxin preparations. • Digoxin's rapid onset of action (30 to 60 minutes) corresponds with peak plasma levels. Maximum effects from a single dose are observed 5 to 6 hours after drug administration, a time at which drug distribution in the body is complete. Digoxin has a steady-state volume of distribution averaging 6.7 L/kg of lean body weight (range, 4 to 9 L/kg). New evidence indicates therapeutic benefit and greater safety by targeting serum concentrations in the range of 0.5 to 1.2 ng/mL
4-Digitalis Glycosides (Digoxin) • Digoxin has a half-life (t½) of 1.6 to 2 days (36 to 40 hours) and is characterized by first-order pharmacokinetics. • With renal impairment, the half-life of digoxin is prolonged, reaching 4.4 days or more in total anuria. At a creatinine clearance of 100 mL/min, the percent eliminated per day is 35%, whereas at a creatinine clearance of 0 (i.e., anuria), the percent eliminated per day is 14%,
5-Other Vasodilating Drugs: Hydralazine and Nitrates • Although ACE inhibitors have become the vasodilator drug of choice, the first vasodilators to be used in patients with HF were: • hydralazine and nitrates. • Hydralazine (Apresoline) is a potent arterial dilating agent that provides symptomatic relief of HF by decreasing arterial impedance (afterload) to left ventricular outflow. • Nitrates (e.g., nitroglycerin [NTG], isosorbide dinitrate, and isosorbide mononitrate) have venous dilating properties that decrease left ventricular congestion (preload). • Used in combination, these two agents have additive benefits in alleviating the symptoms of HF and increasing exercise tolerance.
7-Other Inotropic Agents • Previous doubt about the clinical effectiveness of digitalis derivatives and concern over their potential for toxicity prompted a search for alternative positive inotropic drugs. • IV Dopamine and dobutamine, both of which are sympathomimetics, are commonly used in acute cardiac emergencies, but their use is limited by the need for IVadministration in cardiogenic shock. • Dopamine is more effective as an arterial dilator, especially in the kidney, whereas dobutamine has more potent inotropic properties
Other Inotropic Agents • Amrinone and milrinone, nonsympathomimetic inotropes (phosphodiesterase inhibitors), are associated with an unacceptably high incidence of side effects (thrombocytopenia and increased death rates) when given orally, but are available in parenteral form for short-term use in severe HF via enzyme inhibition results in increased cyclic AMP levels in myocardial cells and thus enhances contractility. Their activity is not blocked by propranolol. • Because they are phosphodiesterase inhibitors, they also act as vasodilators. • All inotropes are relatively contraindicated in diastolic HF.
Calcium Channel Blockers • Amlodipine (Norvasc), felodipine (Plendil), isradipine (DynaCirc), nifedipine (Adalat, Procardia), and nicardipine (Cardene) are examples of calcium antagonists with arterial vasodilating and antispasmodic properties. • They offer the theoretic advantage of being afterload-reducing agents in HF, but their applicability in systolic dysfunction is diminished by negative inotropic effects.