Download
1 / 21
220 likes | 393 Views
Mechanism of Blood Pressure Drugs. By: Duc John Ngo, Joel Thomas, Angus Lee, Jia (Sienna) Feng PHM142 | Week 2 | Tuesday, September 16 th , 2014. PHM142 Fall 2014 Instructor: Dr. Jeffrey Henderson.

E N D
Mechanism of Blood Pressure Drugs By: Duc John Ngo, Joel Thomas, Angus Lee, Jia (Sienna) Feng PHM142 | Week 2 | Tuesday, September 16th, 2014 PHM142 Fall 2014 Instructor: Dr. Jeffrey Henderson
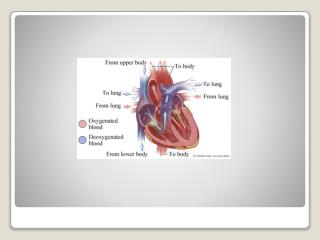
The strength of blood pushing against the side of the vessels while circulating the body • Can be read using a monitor • Normal blood pressure reading 120/80 Ex. 120 - Systolic 80 - Diastolic What is Blood Pressure
AKA Hypertension • NO real symptom present • Only way to identify hypertension is to measure Symptoms of High BP
Also known as Primary Hypertension • Most common type, accounts for 95% of all hypertension cases • Essential Hypertension has no known cause Essential Hypertension
Obesity • Insulin resistance • High alcohol intake • High salt intake • Aging • Sedentary lifestyle • Stress • Low calcium and potassium intake Factors that Increase BP
Also known as nonessential hypertension • Only affects about 5% of cases • Caused by an “identifiable underlying secondary cause” Secondary Hypertension
Renal disorders • Chronic kidney Disease (CKD) • Endocrine disorders • Conn’s syndrome & Cushing’s syndrome • Others • Cancerous tumors, hormonal contraceptives Causes of Secondary Hypertension
Decreasing cardiac outputs • Beta blockers • Diuretics • ACE inhibitors • Decreasing peripheral resistance • Alpha blockers • Diuretics • ACE inhibitors • Calcium Channel Blockers Two Groups of Treatment Methods
[Ca2+] outside of cell membrane, contraction muscles occur with influx of calcium through calcium channels • Blocking channel = no contraction • Reduce contraction of arteries, but increase diameter (vasodilator) • Reduce force of contraction on the heart • Electrical activity within heart = slower heart rate Calcium Channel Blocker (CCB)
Norvasc/Amlodipine • 5 or 10 mg tablet Medication
Angiotensinogen Converting Enzyme Inhibitors (ACEIs) • Angiotensin II type 1 receptor (AT1R) antagonists Renin-Angiotensin-Aldosterone System
Lisinopril (Zestril) • Oral (tablet) • 5 mg, 10 mg, 20 mg Medication
Diuretics: • Decrease peripheral resistance • Thiazides • Carbonic Anhydrase Inhibitors • Loop Diuretics • Potassium sparing diuretics • Osmotic diuretics
filtered 5-10% reabsorbed Sodium in plasma 60-70% reabsorbed 20-30% reabsorbed Carbonic anhydrase inhibitor 1-3% reabsorbed http://www.pathophys.org/diuretics/
Heart attack and heart failure • Stroke on the brain; some cases of dementia • Kidney disease • Limbs are affected leading to peripheral arterial disease affecting legs • Combination of high cholesterol and/or diabetes = bad news Long Term Effect
American Heart Association. “Understanding Blood Pressure Readings.” www.heart.org.N.p., 4 Aug 2014. Web. 13 Sept 2014. http://www.heart.org/HEARTORG/Conditions/HighBloodPressure/AboutHighBloodPressure/Understanding-Blood-Pressure-Readings_UCM_301764_Article.jsp • “amlodipine, Norvasc: Drug Facts, Side Effects and Dosing.” MedicineNet.N.p., 12 Mar 2013. Web. 13 Sept 2014. http://www.medicinenet.com/amlodipine/article.htm • Azizi, Michel, and JoëlMénard. "Combined blockade of the renin-angiotensin system with angiotensin-converting enzyme inhibitors and angiotensin II type 1 receptor antagonists." Circulation 109.21 (2004): 2492-2499. • “Blood Pressure: Calcium channel blockers (CCBs) – blood pressure medication.” Blood Pressure: Blood Pressure UK. N.p., n.d. Web. 13 Sept 2014.http://www.bloodpressureuk.org/BloodPressureandyou/Medicines/Medicinetypes/Calciumblockers • Canadian Pharmacists Association. “Zestril (CPhA Monograph)." e-CPS. CPhA, 2014. Web 13 Sept. 2014.http://www.e-therapeutics.ca.myaccess.library.utoronto.ca/cps.select.preliminaryFilter.action?simplePreliminaryFilter=lisinopril# • Carretero, Oscar A., and Suzanne Oparil. "Essential hypertension part I: definition and etiology." Circulation 101.3 (2000): 329-335. References
Canadian Pharmacists Association. "ACE Inhibitors (CPhA Monograph)." e-CPS. CPhA, 2014. Web. 13 Sept. 2014. https://www.e-therapeutics.ca/tc.showChapter.action?documentId=c0021 • "Diuretics and renal hormones | McMaster Pathophysiology Review." McMaster Pathophysiology Review | MPR | pathophys.org | beta. N.p., n.d. Retrieved from http://www.pathophys.org/diuretics/ on 14 Sept. 2014. • Gray Jean, editor. e-Therapeutics+ [Internet]. Ottawa (ON): Canadian Pharmacists Association; c2007 [cited 2007 Jul 30]. Available from: http://www.e-therapeutics.ca. Also available in paper copy from the publisher. • Guzman, Flavio. “Calcium channel blockers: classification, mechanism of action and indications | CME at Pharmacology Corner.” Medical Pharmacology |Pharmacology Corner. N.p., n.d. Web. 13 Sept 2014. • Hypertension Canada. Canadian Hypertension Education Program (CHEP). 2014 CHEP recommendations. Available from: hypertension.ca/en/chep. Accessed April 24, 2014. • Kenny, Tim. “Medicines for High Blood Pressure, Reduce Blood Pressure | Health.” patient.co.uk.N.p., 23 Jan 2014. Web. 13 Sept 2014. http://www.patient.co.uk/health/medicines-for-high-blood-pressure# • Koeppen, Bruce M, and Bruce A. Stanton. Renal Physiology. Table 4-4, 2013. Print.
"Lisinopril (By mouth) - National Library of Medicine." PubMed Health. Truven Health Analytics, 1 Aug. 2014. Web. 13 Sept. 2014. • Lubel, John S., et al. "Liver disease and the renin–angiotensin system: recent discoveries and clinical implications." Journal of gastroenterology and hepatology 23.9 (2008): 1327-1338. • Omura, Masao, et al. "Prospective study on the prevalence of secondary hypertension among hypertensive patients visiting a general outpatient clinic in Japan." Hypertension research: official journal of the Japanese Society of Hypertension 27.3 (2004): 193-202. • "Understanding Blood Pressure Readings." www.heart.org. N.p., n.d. Web. 13 Sept. 2014.http://pharmacologycorner.com/calcium-channel-blockers-classification-mechanism-of-action-indications/
Summary Slide • Blood pressure –The force of the blood pushing on the walls of the blood vessels while it circulates the body • Systolic pressure is the measured pressure in the blood vessels when the heart muscles contract. Diastolic pressure is the measured pressure in the blood vessels between contractions, when the valves of the heart refill with blood. A systolic value of 120 or less and a diastolic value of 80 or less is considered normal. • Patients with high blood pressure are diagnosed with hypertension. Essential hypertension accounts for 95% of all hypertension cases and the direct cause is unknown. Factors can increase blood pressure such as: obesity, insulin resistance, high alcohol or salt intake, aging, sedentary lifestyle, stress, and low calcium or potassium intake. Nonessential hypertension affects about 5% of cases and is caused by an “identifiable underlying secondary cause” (another medical condition is present and diagnosed). Ex. chronic kidney disease, Conns and Cushing’s syndrome and tumors.There are 2 treatment pathways, decreasing cardiac output (beta-blockers, diuretics and ACE inhibitors) whereas the second group involves decreasing peripheral resistance (alpha-blockers, diuretics, ACE inhibitors and Calcium Channel Blockers. • Calcium channels are on the cell membrane that allows the muscles to contract when an influx occurs with a higher concentration on inside than outside.Calcium channel blocker (CCB) prevents the contraction of the muscles by binding to specific sites of the channel.In doing so, the contraction of arteries and the force placed on the heart is reduced.Muscle lining of arteries are relaxed, which reduces the amount of work the heart has to do in order pump blood.There is a slower heart rate due to a lowering in the electrical activity within the heart. Ex. Norvasc (amlodipine) – works by increasing blood flow to heart (dilating coronary arteries) and blocks the calcium channels preventing calcium flow. • Renin-Angiotensin-Aldosterone System (RAAS) blockers are antihypertensive drugs • Two main types: • Angiotensin Converting Enzyme (ACE) inhibitors – inhibit conversion of Angiotensin I to Angiotensin II • Angiotensin II Receptor 1 Antagonist – Prevent Angiotensin II from binding to the AT1 Receptors • RAAS system is responsible for maintaining fluid balance and blood pressure • -Renin is released by kidney when blood pressure is low. Renin converts angiotensinogen to angiotensin I-> angiotensin II (with ACE) -> binds to AT1 receptors -> Vasoconstriction. -RAAS blockers intercept the cascade at various points to inhibit the formation of angiotensin II • Diureticslower blood pressure by decreasing peripheral resistance. • Types of Drugs: Thiazides, Carbonic Anhydrase Inhibitors, Loop Diuretics, Potassium sparing diureticsand Osmotic diuretics • Thiazidesinhibit the Na+ Cl- co-transporter, inhibiting sodium and chloride ion reabsorption, resulting in increased urine flow from higher sodium excretion and water elimination. • Loop diuretics target Na+ K+ 2Cl- co-transporter at the ascending limb. • .