Download
1 / 19
280 likes | 889 Views
HEPATITIS D VIRUS. Okeke Lotanna #1263. TABLE OF CONTENTS. Definition History Life Cycle Delta antigens Prevalence Cause of disease Risk for infection Stability Symptoms Diagnosis Transmission Treatment And Prevention. DEFINITION.

E N D
HEPATITIS DVIRUS OkekeLotanna #1263
TABLE OF CONTENTS • Definition • History • Life Cycle • Delta antigens • Prevalence • Cause of disease • Risk for infection • Stability • Symptoms • Diagnosis • Transmission • Treatment And Prevention
DEFINITION • Hepatitis is a general term meaning inflammation of the liver and can be caused by a variety of different viruses such as hepatitis A, B, C, D and E. • Since the development of jaundice is a characteristic feature of liver disease, a correct diagnosis can only be made by testing patients' sera for the presence of specific antigens and anti-viralantibodies.
HISTORY • Hepatitis D virus was first reported in the mid-1977 as a nuclear antigen in patients infected with HBV who had severe liver disease • This nuclear antigen was then thought to be a hepatitis B antigen and was called the delta antigen. • Subsequent experiments in chimpanzees showed that the hepatitis delta antigen (HDAg) was a structural part of a pathogen that required HBV infection to replicate. • The entire genome was cloned and sequenced in 1986. It was subsequently placed in its own genus:Deltavirus.
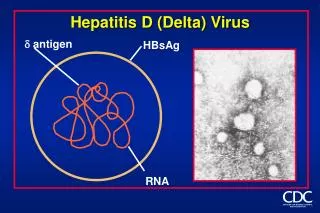
The HDV is a small, spherical virus with a 36 nm diameter. • It has an outer coat containing three HBV envelope proteins (called large, medium, and small hepatitis B surface antigens). • The HDV genome exists as an enveloped, negative sense, single-stranded, closed circular RNA • HDV is the smallest "virus" known to infect animals. • It has been proposed that HDV may have originated from a class of plant pathogens called viroids, which are much smaller than viruses.
LIFE CYCLE • The receptor that HDV recognizes on human hepatocytes has not been identified; however it is thought to be the same as the HBV receptor because both viruses have the same outer coat. • HDV recognizes its receptor via the N-terminal domain of the large hepatitis B surface antigen, HBsAg. • There are eight reported genotypes of HDV with unexplained variations in their geographical distribution and pathogenicity. DELTA ANTIGENS • A significant difference between viroids and HDV is that, while viroidsproduce no proteins, HDV is known to produce one protein, namely HDAg. • HDAg-S (a protein) is produced in the early stages of an infection and enters the nucleus and supports viral replication.
PREVALENCE Areas of high prevalence include the Mediterranean Basin, the Middle East, Central Asia, West Africa, the Amazon Basin of South America and certain South Pacific islands. • Severe, often fatal, acute and chronic type D hepatitis occurs among indigenous people of Venezuela, Colombia, Brazil, and Peru, all regions with high chronic HDV infection rates. • Hepatitis D is less common in Eastern Asia, but is present in Taiwan, China and India
CAUSE OF DISEASE • Hepatitis D or delta hepatitis is caused by the hepatitis delta virus (HDV), a defective RNA virus. • HDV requires the help of a hepadnavirus like hepatitis B virus (HBV) for its own replication. WHO IS AT RISK OF INFECTION • Chronic HBV carriers are at risk for infection with HDV. • Individuals who are not infected with HBV, and have not been immunized against HBV, are at risk of infection with HBV with simultaneous or subsequent infection with HDV. • Since HDV absolutely requires the support of a hepadnavirus for its own replication, inoculation with HDV in the absence of HBV will not cause hepatitis D.
STABILITY • Because of its double-strandedness, the HDV RNA is relatively stable. • The hepatitis delta virus survives dry heat at 60°C for 30h. .
SYMPTOMS • Acute hepatitis D occurs after an incubation period of 3 - 7 weeks. The pre-icteric phase begins with symptoms of : • Fatigue • Lethargy • anorexia and • Nausea • It usually lasts 3 to 7 days. • During this phase, ALT and AST activities become abnormal. • Upon onset of the Icteric Phase, the appearance of jaundice is the typical manifestation. Fatigue and nausea persist, clay-colored stools and dark urine appear, and serumbilirubin levels become abnormal.
DIAGNOSIS • Hepatitis D should be considered in any individual who is HBsAg positive or has evidence of recent HBV infection. • The diagnosis of acute hepatitis D is made after evaluation of serologic tests for the virus. Total anti-HDV are detected by commercially available radioimmunoassay (RIA) or enzyme immunoassay (EIA). ACUTE HBV-HBV INDICATIONS: • Appearance of HBsAgand HBV DNA in serum during incubation. • Appearance of anti-HBc at onset of clinical disease • Appearance of IgM anti-HD, HDV RNA, HDAg in serum • Anti-HDVantibodies develop late in acute phase and usually decline after infection to sub-detectable levels • If HDAg is detectable early during infection, it disappears as anti-HDV appears • All markers of viral replication disappear in early convalescence, and both IgMandIgG anti-HD disappear within months to years after recovery
TRANSMISSION Transmission is similar to that of HBV: • bloodborne and sexual • percutaneous(drug use via injection) • Haemophiliacs • permucosal (sexual)
TREATMENT AND PREVENTION • The vaccine for hepatitis B protects against hepatitis D virus because of the latter's dependence on the presence of hepatitis B virus for it to replicate. • Low quality evidence suggests that interferon alpha can be effective in reducing the severity of the infection and the effect of the disease during the time the drug is given, but the benefit generally stops when the drug is discontinued, indicating that it does not cure the disease. Interferon is effective only in 20% of cases