Download
1 / 19
240 likes | 643 Views
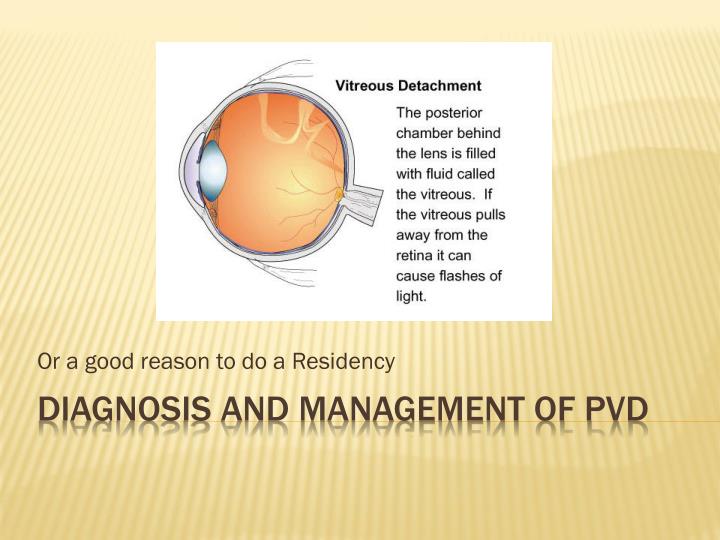
Or a good reason to do a Residency. Diagnosis and management of PVD. Introduction Posterior Vitreous Detachment What it is and why it occurs (anatomy) NOT an obscure entity Clinical diagnosis and management Well established standard of care. PVD. Sources Alexander pp.472-498 (Vitreous)

E N D
Or a good reason to do a Residency Diagnosis and management of PVD
Introduction • Posterior Vitreous Detachment • What it is and why it occurs (anatomy) • NOT an obscure entity • Clinical diagnosis and management • Well established standard of care PVD
Sources • Alexander pp.472-498 (Vitreous) • Review of Optometry • “How To Make Sense of Flashes and Floaters” • “Should I Send Out That PVD” • Clinical Experience • Disease Lab • BIO • Retinal biomicroscopy PVD
Background • Typically after age 45 years • Prevalence = to person’s age over 50 years PVD
Background • Classified as complete (more common) or incomplete • Complete: vitreous gel collapse, vitreous completely separated from sensory retina • Annulus floating in front of optic nerve head • Incomplete: vitreous not completely separated from sensory retina • Macular pulling: edema or hole / metamorphopsia or decreased VA • With or without vitreous collapse PVD
Background • Why is acute symptomatic PVD an ocular emergency? • Increased risk of retinal breaks 8-46%, 15-30% • Usually within 6 weeks after initial onset of symptoms • Think of PVD as dynamic PVD
Background • CE (Cataract Extraction) • May cause a PVD • Shift of ocular contents • Symptoms may be more noticeable after CE • In general, increased risk of retinal detachment after CE • Reason for DFE as part of post-operative regimen PVD
Diagnosis: history • Flashes (photopsia) and floaters • Recent onset / chief complaint • May be a serious, vision threatening problem • Immediate exam (that day) PVD
Small, few in #, linear appearance • Noticeable against bright background • Vitreous degeneration and syneresis • Large floater, may resemble a smoke ring or insect • PVD • Aging: lacunae(pockets of liquefied vitreous) accumulate, vitreous body loses support, vitreous framework contracts • Liqufied vitreous escapes to retrohyaloid space • Vitreous separated completely from sensory retina Floaters: history
Large floater, may resemble a smoke ring or insect • You see an annual ring (where posterior vitreous attaches to optic nerve head) • Ring floats over posterior pole • Patient describing the shadow from the annulus • Small floaters, may enlarge and appear red or purple to the patient • Vitreous heme: with PVD, neovascularization • Multiple floaters with decreased VA • Inflammed retina and choroid with vitritis • Debris within pre-corneal tear film? Floaters: History
Why: mobile vitreous mechanically pulls or tugs on retina stimulation of photoreceptors signal sent to occipital cortex perceived as a flash • Possible causes: • Retinal tear / detachment • PVD • Migraine prodrome • A general comment: Patients with retinal detachementsMAY NOT report a history of flashes of floaters. Flashes : History
Diagnosis: exam • Dilated fundus exam • BIO: posterior pole shadow • Scleral depression • Retinal biomicroscopy: vitreous • Red blood cells / pigment cells: retinal detachment • White blood cells: inflammation or tumors • Record techniques performed PVD
Diagnosis: exam • Dilated fundus exam: looking for? • PVD • Holes, tears, RD • VF? • Full field • Recent detachment associated with relative scotoma PVD
Management • Most do not require retinal consultation • Based on your capabilities (skills) with the patient, how difficult exam was, and patient history • Red flags for referral • Vitreal red blood cells or pigment • Lattice degeneration? • Patient difficult to examine: media opacity or limited pupil dilation • No reason for flashes / floaters of recent onset PVD
Management • Uncomplicated PVD and appropriate O.D. • RTC 1 month: DFE + • Highest risk of associated holes, tears, RD • Then RTC 3-6 months: DFE + • Lower risk of complications after a few months • Every case is unique (Alexander: 1-4 weeks, then 1 month later) • Education • RTC immediately if noting increase in # of flashes or floaters, shadow in vision, decreased VA PVD
Management: Education / “Real Patient Care” • With time, “flashes decrease and floaters less noticeable” • “Normal aging change associated with a more watery gel between the front and back of the eye” • Importance of RTC and symptoms of complication PVD
Rare, more obscure Vitreous base attachement anteriorly very very strong Lens dislocation, trauma Marfan syndrome or homocystinuria Anterior vitreous detachment
Still have not sold my house You may be wondering why Asking for your opinion regarding my neighborhood and home? My memphis house situation