Download
1 / 42
420 likes | 593 Views
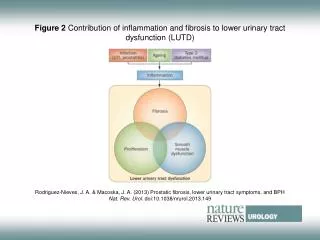
Interplay of subclinical fibrosis and inflammation. D. Serón Nephrology Department Hospital Vall d’Hebron Barcelona. Surveillance biopsies. Inflammation with and without fibrosis. Inflammation and CHR. Innate immunity and inflammation. Surveillance biopsies.

E N D
Interplay of subclinical fibrosis and inflammation D. Serón Nephrology Department Hospital Vall d’Hebron Barcelona
Surveillance biopsies Inflammation with and without fibrosis Inflammation and CHR Innate immunity and inflammation
Surveillance biopsies Inflammation with and without fibrosis Inflammation and CHR Innate immunity and inflammation
Inflammation and fibrosis in surveillance Bx Fibrosis Graft survival Graft survival Inflammation Dimény E, Clin Transplantation 1995; 58(11): 1195 Serón D, Kidney Int 1997; 51: 310 Nankivell BJ et al, Transplantation 2004; 78:242 Choi BS et al, Am J Transplant 2005; 5: 1354
SCR and CAN in paired biopsiesn=598 Bx, (no SCR 462, SCRB 102, SCRA 34) * p<0.05 ***p<0.001 Nankivell BJ et al, Transplantation 2004; 78:242 Ibernon et al et al, Kidney Int 2006; 76: 557
Proper classification of inflammation and fibrosis Normal (no inflammation no fibrosis) Inflammation (no fibrosis) Fibrosis (no inflammation) Inflammation and fibrosis
1 Normal=186 SCR=74 .75 IF/TA=110 IF/TA+SCR=65 .5 .25 months 0 50 100 150 200 SCR & IF/TA SCR + IF/TA 1 year protocol Bx Normal SCR + IF/TA 1 year protocol Bx IF/TA without SCR IF/TA without SCR IF/TA with SCR IF/TA with SCR SCR + IF/TA < 6 month protocol Bx Shishido et al, JASN 2003; 14: 1046 Cosio FG et al, Am J Transplant 2005; 5: 2464, Moreso F et al Am J Transplant 2006; 6:747
High inflammation CD45 CD3 CD20 CD68 CD15 Low inflammation Inflammation with or whitout IF/TA High (upper tertile) and low (two lower tertiles) inflammation Moreso F et al. AJT 2007; 7: 2739
2500 1500 2000 1200 900 1500 CD45 positive cells / mm2 interstitium CD3 positive cells / mm2 interstitium 1000 600 500 300 0 0 NORMAL SCRa IF/TA SCR+IF/TAa,c NORMAL SCRa IF/TA SCR+IF/TAa,c 800 3500 3000 600 2500 CD20 positive cells / mm2 interstitium CD68 positive cells / mm2 interstitium 2000 400 1500 1000 200 500 0 0 NORMAL SCR IF/TAa SCR+IF/TAa,b,c NORMAL SCRa IF/TA SCR+IF/TAa,c Interstitial infiltrating cells Moreso F et al. AJT 2007; 7: 2739
Survival (%) 1 T1 T2 T3 ,8 ,6 ,4 ,2 0 0 20 40 60 80 100 120 140 months Renal allograft survival(univariate) P=0.001 Moreso F et al Am J Transplant 2006; 6: 747
Renal allograft survival(multivariate) Variable Univariate Multivariate RR (95% CI) p RR (95% CI) p Retransplant (yes) 2.5 (0.9-6.9) 0.06 1.2 (0.3-5.3) ns PRA > 50% 4.6 (1.7-12.6) <0.01 4.5 (1.0-20.4) 0.05 CD20 (upper tertile) 3.3 (1.4-8.3) <0.01 3.0 (1.2-7.3) 0.01 Moreso F et al Am J Transplant 2006; 6: 747
B cells, acute rejection and outcome inindication biopsies B cells associated with poor outcome in AR Sarwal et al. et al. NEJM 2003; 349: 125. Hippen BE et al. Am J Transplant 2005; 5: 2248 Alausa M et al. Clin Transplant 2005; 10: 137 Eileen WT et al. Transplantation 2006; 82: 1769 Lehnhardt et al. Am J transplant 2006; 6: 847 Zarkhin V et al. Kidney Int 2008; 74: 664 Mourah MR et al. Pediatr Transplant 2009; 13 B cells not associated with poor outcome in AR Scheepstra C et al. Transplantation 2008; 86:772 Bagnasco SM et al. Am J Transplant 2007; 7: 1968-1973
Immunophenotype in protocol biopsies from TAC vs CsA treated patientsn= 44TAC vs 22 CsA P<0.01 ns P<0.01 P<0.05 Serón D et al, Transplantation 2007; 83:649
B cell survival in CHR after rituximabn=38 explanted grafts with CHR 2 after treatment with rituximab Intragraft B cells BAFF positivity Thaunat et al. Transplantation 2008; 85:1648
SCR vs SCR+IF/TA and FoxP3 SCR SCR + No IF/TA IF/TA p N 19 18 ___________________________________________________ %FoxP3 + cells 14.2 +/-16.3 8.2+/-8.1 0.035 ___________________________________________________ Bestard et al. JASN 2008; 19: 2010
T regs in pts ACR and BL (indication (12 ACR, 12 BL) and surveillance (8ACR, 8 BL) Taflin et al. Transplantation 2010; 89: 194
Surveillance Bx cytokine transcripts P< 0.01 Hueso M et al. Am J Pathol 2010; 176: 1696
Inflammation+IFTA B cells Tregs IL10 Ag presentation Th2 response Persistent inflammation? CHR?
Surveillance biopsies Inflammationwith and without fibrosis Inflammation, IF/TA and CHR Innate immunity and inflammation
SCR and CHR Tx Inflammation CAN ± Inflammation Survival
SCR and CHR Tx Inflammation IF/TA ± Inflammation Survival CHR
SCR and Chronic humoral rejection1988-2006 Protocol Bx n = 517 CHR 44 IF/TA nos 42 Recurrence 11 De novo GN 7 Acute rejection 4 Polyoma 1 Bx for cause: n = 109
Variable CHR (44) IF/TA (42) p Protocol biopsy Time (m) 4.5 ± 2.4 4.6 ± 3.3 ns SCr (mol/L) 149 ± 37 144 ± 44 ns Proteinuria (g/d) 0.3 ± 0.2 0.3 ± 0.2 ns Biopsy for cause Time (y) 6.4 ± 3.4 8.2 ± 4.4 0.037 SCr (mol/L) 240 ± 141 204 ± 80 ns Proteinuria (g/d) 2.3 ± 2.4 1.4 ± 1.7 0.061 Clinical characteristics at the time of biopsy
Clinical characteristics of patients Variable CHR IF/TA p-value (n=44) (n=42) __________________________________________________ Donor age (years) 40 ± 16 34 ± 15 ns Donor gender (% male) 65.9 78.6 ns Patient age (years) 43 ± 12 40 ± 12 ns Patient gender (male) 59.1 69.0 ns PRA (%) 7 ± 18 3 ± 10 ns Virus hepatitis C 18.2 9.5 ns Re-transplants (%) 15.9 2.3 0.058 HLA DR mm 0.7 ± 0.5 0.7 ± 0.6 ns Cold ischemia time (hours) 23 ± 6 21 ± 6 ns Immunosuppression CNI without MMF 24 27 CNI with MMF 18 12 CNI with mTOR-i 1 2 CNI free 1 1 ns Delayed graft function (%) 25 19 ns Acute rejection (%) 22.7 26.2 ns _________________________________________________________
Acute Banff score in surveillance Biopsies (p=0.003) Acute score
SCR, CHR and IF/TA CHR IF/TA p __________________________________ SCR (%) 52.3 28.6 0.025 __________________________________ RR 95% CI p __________________________________ SCR 2.52 1.1-6.3 0.047 ReTx 6.7 0.8-58.8 ns __________________________________
% of cases with CHR and IF/TA in the biopsy for cause Dg category in surveillance Bx n=17 n=34 n=17 n=18
Surveillance biopsies Is inflammation in SCR differentfrom SCR + IFTA? Are early Bx findings different in patients developing IFTA in comparison with patients developing CHR Innate immune alterations and inflammation
Risk factors associated with early inflammation in surveillance biopsies Immunosuppressive treatment Acute rejection before surveillance Bx Innate immunity & inflammation in the general population
TLR-2 expression in 6 m surveillance Bx is associated wit lower SCR257 surveillance Bx 6w, 3m, 6m and 108 indication Bx De Groot K et al. Am J Nephrol 2008; 28: 583
MBL 96KDa protein made of 3 identical 32 KDa structures N-acetylglucosamine D-mannose N-acetyl mannosamine L-fructose Carbohydrate recognition domain Collagen like domain N-terminal cross linking region Bouwman LH et al. 2006; 67:247
Defense collagens Bohlson SS et al. Mol Immunol 2007; 44:33
MBL in Renal TransplantsMar 2005 –Oct 2006, 125 RT, 111 with a functioning graft at 3 m T 1 Low MBL N=42 T 2,3 High MBL N=83 Log MBL (ng/ml)
sTNFR2 before Txsoluble TNFR p=0.05 Ibernon M et al. Transplantation 2009: 88: 272
MBL and infection (bacterial or fungal)March 2005-Oct 2006, 125 pts, 111 with a functioning graft at 3 m Ibernon M et al. Transplantation 2009: 88: 272
MBL and NODAT March 2005-Oct 2006, 125 pts, 111 with a functioning graft at 3 m Ibernon M et al. Transplantation 2009: 88: 272
Low MBL and SCR(n=60) P=0,0054 Ibernon M et al. Kidney Int (in press)
Low MBL, subclinical rejection and Tx CAD (N=6) (N=32) Arnt RF et al. Eur Heart J 2005; 26: 1660
C1q and MBL and rejection Bohlson SS et al. Mol Immunol 2007; 44:33
C1q deficiency and acute rejectionHeart transplant in C1q deficient mice WT C1q-/- Csencsits K et al. AJT 2008; 8: 1622
C1q deficiency and acute rejectionHeart transplant in C1q deficient mice T cell response is not enhanced in C1q-/- mice More intense anti-donor Ab response Csencsits K et al. AJT 2008; 8: 1622
Tissue injury and repair Repair Normal IFTA - Innnate Immunity Inflammation (SCR) Tx Injury Apotosis Necrosis Progression of injury SCR + IFTA CHR +