Download
1 / 35
350 likes | 377 Views
Learn how to assess the renal system physically and understand the diagnostic tests involved, such as urinalysis, Creatinine clearance, and renal angiography. Proper preparation and instructions for each test are provided for effective patient care.

E N D
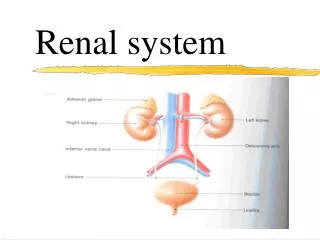
Renal system (physical assessment) • Inspection: Skin- pallor, yellow-gray, excoriations, changes in turgor, bruises, texture(e.g. rough, dry skin) • Mouth: stomatitis, ammonia breath. • Face & extremities- generalized edema, peripheral edema, bladder distention, masses, enlarged kidney. • Abdomen-abdominal contour for midline mass in lower abdomen (may indicate urinary retention) or unilateral mass. • Weight: weight gain 2nd to edema, weight loss & muscle wasting in renal failure.
Renal system (physical assessment) • General state of health- fatigue, lethargy, & diminished alertness. • Palpation- No costovertebral angle tenderness, nonpalpable kidney & bladder, no palpable masses. • Percussion: Tenderness in the flank may be detected by fist percussion. If CVA tenderness & pain are present, indicate a kidney infection or polycystic kidney disease. • Auscultation: The abdominal aorta & renal arteries are auscultated for a bruit, which indicates impaired blood flow to the kidneys
Renal Systems (Diagnostic test) • Urinalysis-evaluation of the renal system & for determining renal disease. • Wash perineal area & use a clean container. • Obtain 10 to 15 mL of the 1st AM sample • If the client is menstruating, indicate this on the lab. requisition form. • Specific Gravity-measures the kidney’s ability to concentrate urine. Measured by multiple-test dipstick (most common method), refractometer-instrument used in the lab, urinometer (least accurate method). Cold specimens produce a false high reading. Factors that interfere with an accurate reading include radiopaque contrast agents, glucose & proteins.
Renal Systems (Diagnostic test) • A decrease in SG (less conc. urine) occurs with increased fluid intake, diuretic administration, diabetes insipidus. • An increase SG (more conc. Urine) occurs with insufficient fluid intake, decreased renal perfusion, or the presence of ADH. • Urine Culture & Sensitivity- identifies the presence of microorganisms & determines the specific abx. that will treat the existing microorganisms. Note that urine from a client who forced fluids may be too dilute to provide a positive culture.
Renal Systems (Diagnostic test) • Creatinine clearance test- A blood & timed urine specimen that evaluates kidney function. • Blood is drawn at the start of the test & the AM of the day that the 24-hour urine specimen collection is complete. Maintain the urine specimen on ice or refrigerate. If the client is taking steroids, check with MD regarding the administration of these medications during test. Encourage adequate fluids before & during the test.
Renal Systems (Diagnostic test) • Vanillymandelic acid (VMA)-to diagnose pheochromocytoma, a tumor of the adrenal gland. The test identifies an assay of urinary catecholamines in the urine. Instruct to avoid foods such as caffeine, cocoa, cheese, gelatin at least 2 days prior to beginning of the collection & during collection. Save all urine on ice or refrigerate. Instruct to avoid stress & to maintain adequate food & fluids during the test.
Renal Systems (Diagnostic test) • Uric acid- A 24-hour collection to diagnose gout & kidney disease. • Encourage fluids & a regular diet during testing. Place the specimen on ice or refrigerate. • KUB (Kidney, ureters, bladder) radiograph-An x-ray film that views the urinary system & adjacent structures; used to detect urinary calculi. • Bladder ultrasonography-A noninvasive method of measuring the volume of urine in the bladder.
Renal Systems (Diagnostic test) • Computed tomography (CT) & MRI- provide cross-sectional views of the kidney & urinary tract. • Intravenous pyelogram (IVP)- the injection of a radiopaque dye that outlines the renal system. Performed to identify abnormalities in the system. Withhold food & fluids after midnight before the test. Inform the client abt. Possible throat irritation, flushing of the face, warmth or salty taste that may experienced during the test.
Renal Systems (Diagnostic test) • Renal angiography- the injection of a radiopaque dye through a catheter for examination of the renal arterial supply. Assess the client for allergies to iodine, seafood & radiopaque dyes. Inform about possible burning feeling of heat along the vessel when the dye is injected. • NPO after MN on the night of the test. Instruct to void immediately before the procedure. Inspect the color & temperature of the involved extremities. Inspect site for bleeding.
Renal Systems (Diagnostic test) • Renal Scan- An IV injection of a radiopaque for visual imaging of renal blood flow. Instruct that imaging may be repeated at various interval before the test is complete. Assess for signs of delayed allergic reactions, such as itching & hives. • Cystometrogram (CMG)- A graphic recording of the pressures exerted at varying phases of the bladder. Inform of the voiding requirements during & after the procedure.
Renal Systems (Diagnostic test) • Cystoscopy & Biopsy- the bladder mucosa is examined for inflammation, calculi or tumors by means of a cystoscope, a biopsy may be obtained. NPO after MN before the test. Monitor for postural hypotension. Note that pink-tinged or tea-colored urine is common. Monitor for bright, red or clots & notify MD. • Renal biopsy- insertion of a needle into the kidney to obtain a sample of tissue for exam. NPO after MN. Provide pressure to the biopsy site for 30 minutes. Check site for bleeding. Force fluids to 1500-2000 mL. Instruct to avoid heavy lifting & strenuous activity for 2 weeks.
Urinary Tract Infection (UTI) • Inflammation of the bladder from infection or obstruction of the urethra. • The most common causative organism are E. coli, Enterobacter, pseudomonas, & serratia. • More common in women because they have shorter urethra than men, & the location of the urethra in women is close to the rectum. • Sexually active & pregnant women are most vulnerable to UTI.
Urinary Tract Infection (UTI) • Causes: Allergens or irritants, such as soaps, sprays, bubbles bath • Bladder distention, calculus, hormonal changes influencing alterations in vaginal flora. • Indwelling urethral catheter, loss of bacterial properties of prostatic secretions in the male • Sexual intercourse, urinary stasis, use of spermicides, wet bathing suits
Urinary Tract Infection (UTI) • Assessment: Frequency & urgency, burning on urination, voiding in small amount, inability to void, incomplete emptying of the bladder, lower abdominal discomfort or back discomfort, cloudy, dark, foul smelling urine, hematuria, bladder spasms, malaise, chills, fever, nausea & vomiting. • Implementation: Obtain urine C/S to identify bacterial growth. Instruct to force fluids up to 3000 mL a day. Provide meticulous perineal care with an indwelling catheter. Instruct to avoid alcohol. Provide heat to abdomen or sitz bath for complaints of discomfort
Urinary Tract Infection (UTI) • Nursing Diagnosis: Acute pain r/t inflammation of mucosal tissue of UT as manifested by pain on urination, flank pain, bladder spasms. • Provide relief by administering analgesics such as Pyridium or combination agents (Urised). Alert that urine color will be orange & blue or green with combination agents. • Teach the use of nonpharmacologic technique- heating pad, warm showers.
Urinary Tract Infection (UTI) • Impaired urinary elimination r/t UTI as manifested by bothersome urgency, hematuria or concern over altered elimination pattern • Obtain midstream voided specimen for C/S. • Administer antimicrobial drugs. • Teach signs & symptoms of UTI. • Encourage adequate fluid to help prevent infection and dehydration.
Urolithiasis • Formation of urinary stones; urinary calculi formed in the ureters. • When a calculus occludes the ureter & blocks the flow of urine, the ureter dilates, producing a condition known as hydroureter. • If the obstruction is not removed, urinary stasis results in infection, impairment of renal function on the side of the blockage, & resultant hydronephrosis & irreversible kidney damage.
Urolithiasis • Causes: Family history of stone formation • Diet high in CA, vitamin D, milk, protein, purines • Obstruction & urinary stasis • Dehydration • Use of diuretics, which can cause volume depletion • Immobilization • Hypercalcemia, & hyperparathyroidism • Elevated uric acid, such as gout
Urolithiasis • Nursing Assessment: Nausea, vomiting, dietary intake of purines, phosphates, low fluid intake; chills. • Elimination: Decreased u/o, urinary urgency, feeling of bladder fullness. • General: Acute, severe colicky pain in flank, back, abdomen groin or genitalia; burning sensation on urination, dysuria,anxiety. • Skin: warm, flushed skin or pallor with cool. • Urinary: tenderness on palpation on renal areas, passage of stone(s). • Increased BUN & creatinine; WBC, calcium, phosphorus, uric acid. • KUB- calculi or anatomic changes on IVP
Urolithiasis • Implementation: Force fluids up to 3000 mL/day, unless contraindicated-to facilitate the passage of the stone & prevent infection. • Strain all urine for the presence of stones. • Turn and reposition immobilized clients. • Administer analgesics & response to pain. • Instruct in the diet specific to the stone composition.
Urolithiasis • Surgical therapy: • Nephrolithomy- incision into the kidney to remove the stone. • Pyelolithotomy- incision into the renal pelvis to remove the stone. • Ureterolithotomy-removal of stone in the ureter. • Cystotomy- indicated for bladder calculi. • Lithotripsy- procedure used to eliminate calculi in the kidney. Hematuria is common after the procedure. A stent is often placed after the procedure to promote passage and to prevent obstruction, then removed 1 to 2 weeks after lithotripsy.
Urinary Tract Infection (UTI) • Teaching: teach good perineal care & to wipe from front to back. • Instruct to void every 2 to 3 hours. • Instruct to void & drink a glass of water after intercourse. • Encourage menopausal women to use estrogen vaginal creams to restore pH. • Instruct the female to use water- soluble lubricants for coitus, especially after menopause.
Polycystic Kidney Disease • A cystic formation and hypertrophy of the kidney, which lead to cystic rupture, infection, formation of scar tissue and damaged nephrons. • The ultimate results of this disease is renal failure. • Types: Infantile: inherited autosomal recessive trait that results in the death of the infants within few month after birth. • Adult: dominant trait results in end-stage renal disease.
Polycystic Kidney Disease • Assessment: Flank lumbar pain or abdominal pain, fever, chills, UTIs, hematuria, proteinuria, pyuria HTN, palpable abdominal masses & enlarged kidney. • Implementation: • Monitor for gross hematuria which indicates cyst rupture. • Increase sodium & water loss intake because sodium loss rather than retentions. • Provide bed rest if cyst ruptured & bleeding occurs
Polycystic Kidney Disease • Implementation: Prepare for percutaneous cyst puncture for relief of obstruction or draining an abscess. • Prepare client for dialysis and encourage genetic counseling.
Renal Tumors • May be benign or malignant: Common sites of metastasis include bone, lungs, liver, spleen or other kidney. • Assessment: Dull flank pain, palpable renal mass, painless hematuria. Unknown cause. • Treatment: Radical nephrectomy: Removal of the entire kidney, adjacent adrenal gland & renal artery & vein. • Radiation therapy & chemotherapy.
Renal Tumors • Implementation: Monitor abdomen for distention caused by bleeding • Observe bed linens under the client for bleeding • Monitor for hypotension, decreases in urinary output & alterations in LOC, indicating hemorrhage. • Monitor urinary ouput • Do not irrigate or manipulate the nephrostomy tube if in place.
Nephrotic Syndrome • Arising from protein wasting 2nd to diffuse glomerular damage. • Assessment: Proteinuria, edema, anemia,, malaise, irritability, HTN, waxy pallor of the skin, amenorrhea or abnormal menses. • Implementation: Monitor I/O. Bedrest if edema present, monitor daily weights. • Administer plasma expanders, to raise the osmotic pressure.
Nephrosclerosis • Sclerosis of the small arteries & arterioles of the kidney. There is decreased blood flow, which results in patchy necrosis of the renal parenchyma. • Benign –occurs in adults 30 to 50 yrs. of age. It is caused by vascular changes resulting from hypertension and from atherosclerosis process. • Malignant-complication of HTN,characterized by sharp increase in BP with a diastolic pressure greater than 130 mm Hg. • Treatment- aggressive antihypertensive therapy. The prognosis is poor.
Phases of ARF • Oliguric phase: GFR decrease,hyperkalemia, fluid overload, elevated BUN & creatinine. • Diuretic phase: GFR Begins to increase, hypokalemia, hypovolemia, gradual decline in BUN, creatinine. • Recovery phase: BUN is stable & normal, complete recovery may take 1 to 2 years.
Stages of Chronic RF • Stage 1: Diminished renal reserve-renal function is reduced, no accumulation of metabolic wastes, nocturia & polyuria occurs as a result of decreased ability to concentrate urine. • Stage 11: Renal Insufficiency: metabolic waste begin to accumulate, oliguria & edema occur as a result of decreased responsiveness to diuretics. • Stage 111: excessive accumulation of metabolic waste. Kidney are unable to maintain homeostasis. Dialysis is required.
Kidney Transplant • Implantation of a human kidney from a compatible donor into a recipient. • Performed for irreversible kidney failure. • Immunosuppressive medications must be taken for life. • Complications: Graft rejection- fever, malaise, elevated WBC, graft tenderness, signs of deteriorating renal function, acute HTN, anemia. Occurs immediately after surgery to 48 hours-removal of rejected kidney.
Kidney Transplant • Avoid prolonged period of setting • Recognize the signs & symptoms of infection & rejection. • Avoid contact sports • Use medications & maintained immunosuppressive therapy for life.