Download
1 / 23
230 likes | 357 Views
GNRS 5521: Clinical Care Practicum By: Deanne Garay. Health promotion: antidepressant wean. Demographics . Identifying Data. J. D. 52 year-old Hispanic Male Primary caregiver Known patient to clinic Reliable source based on memory, trust, and mood. Subjective Data . Chief Complaint.

E N D
GNRS 5521: Clinical Care Practicum By: Deanne Garay Health promotion: antidepressant wean
Demographics Identifying Data • J. D. • 52 year-old • Hispanic Male • Primary caregiver • Known patient to clinic • Reliable source based on memory, trust, and mood
Subjective Data Chief Complaint • “Medication refills, 3 month follow-up, interest in weaning off depression medications.”
Current Health Status • Allergies: NKDA • Medications: Lisinopril 20 mg PO QD; HCTZ 12.5 mg PO QD; Amlodipine 5 mg PO QD; TriCor 145 mg PO QD Venlafaxine75 mg PO QD. • Immunizations Status: Childhood immunizations are UTD. Received annual flu shot. • Habits: Drinks alcohol on the weekends (about 4 beers), smokes tobacco (1 PPD) and denies the use of illicit drugs. He drinks about 4 cups of coffee every morning. • Health Maintenance Practices: • Last Physical Exam: 3 months ago in this clinic • Colonoscopy: 2011 • Self Testicular Exam: Reports
Subjective Data Relevant Past Medical History • Has been diagnosed with HTN, Depression, Anxiety, & Hyperlipidemia • Hospitalizations/Surgeries: Appendicitis when he was 12 • Other: Denies other emergency room visits, blood transfusions, or serious accidents or injuries in his life.
Subjective Data Social History • Home living conditions: Lives in a house with wife and 15 year old daughter • Occupation: Owns and manages own successful local restaurant • Economic Status: Has private insurance with no economic concerns. • Military Record: N/A • Religious/cultural: No religious or cultural considerations that would affect his care.
Subjective Data Family History • Father passed away when he was 74 from colon cancer, had high blood pressure. • Mother is living, 79, has high blood pressure, diabetes mellitus, & high cholesterol. • Older brother, 57, is living and has high blood pressure, and high cholesterol. • Younger sister, 49, is healthy with no known medical conditions.
Subjective Data Patient’s Explanatory Model • Patient states that things have “calmed down” with his business and he would like to try to wean off of venlafaxin.
Subjective Data Relevant Review of Systems • GENERAL: Has been feeling “good,” and denies any recent weight changes. Reports low fat, low CHO diet. Increased salads and low fat dressings once/day. Started drinking protein shakes. Denies any malaise, chills, or fever. He states that he is sleeping better now that the stress of the restaurant has decreased. • CHEST/LUNGS: Denies cough, wheezing and shortness of breath. Reports tobacco use (1 PPD x20 years) • CV: Denies chest pain, discomfort, palpitations, and edema, dyspnea or orthopnea. Reports HTN controlled on medications. He monitors on home monitor and gets BP’s ranging 118-120’s/75-80’s. Has been taking TriCor for high cholesterol.
Subjective Data Relevant Review of Systems (Continued) • GI: Denies trouble swallowing, heartburn, abdominal pain, nausea, vomiting or diarrhea. • MSK: Denies any muscle aches or pains. For exercise he walks with wife around neighborhood 3 days out of the week (weather permitting). On feet a lot for work. • PSYC: Reports decreased stressors and feels that he has developed better coping mechanisms.
Objective Data Physical Exam • GENERAL/CONSTITUTIONAL: J.D. is an obese, middle-aged man. Well nourished, cooperative and in no acute distress. • VITAL SIGNS: Temp 98.4 PO; RR 18; HR 82; BP 120/78 Ht-67 in; Wt-220lbs; BMI-34.5 • PSYC: Alert & Oriented to person, place & time. Recent and remote memory intact. Mood and affect appropriate for situation. Judgment & insight normal. Normal attention span and concentration. Pleasant, smiling, calm. • NECK: Supple, Thyroid normal, No regional lymphadenopathy, no masses, No carotid bruits.
Objective Data Physical Exam(Continued) • CHEST/LUNGS: Respiratory effort unremarkable. RR and pattern normal. Lungs clear to auscultation, bilaterally. • CV: HR and Rhythm normal. Normal S1, S2. No murmurs, rubs, gallops, or clicks. Extremities warm and peripheral pulses normal and palpable. No cyanosis, rash, or clubbing noted. Cap refill <2 seconds. No peripheral edema. • GI: Abdomen round. Bowel sounds present x4 quadrants. No bruits noted. No tenderness or masses noted. No hepatosplenomegaly or ascites noted. • MSK: Normal station and gait.
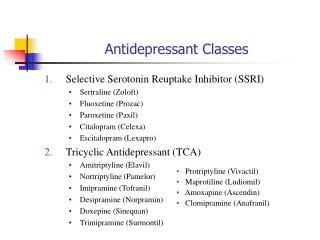
Assessment Diagnoses • 401.9 – Unspecified essential hypertension • 272.4 – Other and unspecified hyperlipidemia • V58.69 – Long-term (current) use of other medications • 311 – Depressive disorder, not elsewhere classified • 305.1 – Tobacco use disorder
Diagnosis 311 – Depressive disorder • “Depression is a constellation of signs and symptoms that is an abnormal reaction to life’s difficulties. Disturbances in cognitive, emotional, behavioral, and somatic regulations are involved. Depressed mood, and loss of interest or pleasure are the major symptoms,” (Hollier, 2011, p. 653). • “Virtually every class of medication includes some agent that can induce depression. Antihypertensive drugs, anticholesterolemic agents, and antiarrhythmic agents are common triggers of depressive symptoms,” (Longo et al, 2012, p. 3536).
Plan Diagnostics • Labs: • CMP: WNL except Glucose 138 (needs 3 hour gtt) • Lipid Panel: • Total Cholesterol 174 • HDL 30 • TRIG 219 • (Trigs high but cholesterol improved from last visit)
Plan Therapeutics • Continue medications as previously prescribed: • Lisinopril 20 mg PO QD • Amlodipine 5 mg PO QD • HCTZ 12.5 mg PO QD • TriCor 145 mg PO QD
Plan Therapeutics • Venlafaxine Wean • Current dose: 75 mg ER PO QD • Decrease by 37.5 mg PO every other day, weekly, until completely weaned off
Plan Venlafaxine • No trade name (used to be Effexor) • Class: SNRI’s (Mixed Norephinephrine/Serotonin Reuptake Inhibitor & Receptor blocker) • Indication: MDD, GAD, Social phobia, Panic Disorder, Vasomotor symptoms • Adverse Reactions & Prescribing Considerations: Monitor BP due to potential emergent HTN, Insomnia & nervousness, weight loss, may increase cholesterol (Dunphy, 2011) • Black Box Warning: Suicidality • Taper dose by no more than 75 mg/wk to D/C
Plan Venlafaxine wean • “When the patient reports target symptom relief or the assessment indicates symptom remission has been achieved, the practitioner and patient develop a treatment discontinuation plan,” (Dunphy, 2011, p. 1039). • “Antidepressant medications should be tapered rather than abruptly discontinued,” (Hollier, 2011, p. 659). • Withdrawl side effects include flu-like and GI symptoms (Dunphy, 2011).
Plan Education and Counseling • Weaning schedule for venlafaxine • Importance of interpersonal relationships • Low fat, low cholesterol diet • Encouraged smoking cessation • Cautioned that alcohol may exacerbate depressive symptoms
Plan Follow-up Care • The patient was instructed to follow-up in 3 monthsto evaluate psychological status and for fasting labs and glucose or sooner for withdrawal symptoms. • The patient was provided community resources and emergency numbers.
Update Follow-up • Patient returned in about 1 month anxious and requesting more medication. • Resumed 75 mg venlafaxine ER PO QD. • Repeated CMP for glucose check. (pending results) • Follow up as scheduled (for 3 month check) to reevaluate • “Regardless of the treatment undertaken, the response should be evaluated after ~2 months. Three-quarters of patients show improvement by this time, but if remission is inadequate the patient should be questioned about compliance and an increase in medication dose should be considered if side effects are not troublesome. If this approach is unsuccessful, referral to a mental health specialist is advised,” (Longo et al, 2012, p.3539)
References • Dunphy, L.M., Winland-Brown, J.E., Porter, B.O., & Thomas, D. J. (Eds.). (2011). Primary care: The art and science of advanced practice nursing (3rd ed.). Philadelphia: F.A. Davis. • Hollier, A., Hensley, R. (2011). Clinical Guidelines in Primary Care: A reference and review book. Lafayette: Advanced Practice Education Associates, Inc. • Longo, D., Kasper, D., Jameson, J.L., Fauci, A.S., Hauser, S.L., & Loscalzo, J. (2012). Harrison’s Principles of Internal Medicine (18thed). New York: McGraw Hill Medical