Download
1 / 28
300 likes | 633 Views
EPIDEMIC CEREBROSPINAL MENINGITIS. Dept. Of Infectious Disease Shengjing Hospital. DEFINITION. 1. Epidemic cerebrospinal meningitis is acute infectious disease caused by meningococcus. 2.characteristics of ECM are fever,

E N D
EPIDEMIC CEREBROSPINAL MENINGITIS Dept. Of Infectious Disease Shengjing Hospital
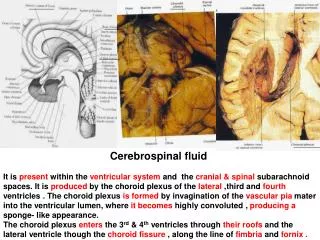
DEFINITION • 1. Epidemic cerebrospinal meningitis is acute infectious disease caused by • meningococcus. • 2.characteristics of ECM are fever, • headache, vomiting , petechiae or ecchymosis , and meningeal irritation signs. CSF is purulent .
ETIOLOGY • 1.Pathogen is Neisseria meningitidis (meningococcus); G- diplococcus. • 2.Biological features: • 2.1.The organism grow by incubation • on blood,chocolate or trypticase soy agar in 5~10%CO2,PH 7.4~7.6; • 2.2.The organism is susceptible to dry, • heat , chill and disinfectant;
ETIOLOGY • 2.3. autolysis by autolysin in vitro; • 3.The organism can be detected in patient’s nasopharynx, blood, CSF, petechiae in skin; • 4.Pathogenic factor: endotoxin.
ETIOLOGY • 5.Serogroups of meningoccus; • 13 serogroups and more than 20 serotypes found in the world; • most common serogroups: • A B C group • Group A is the most common in china.
EPIDEMIOLOGY • 1.Source of infection: • patients and carriers; • 2.The routes of transmission : • 1) air borne • 2) closed contact transmission : • 3.Susceptibility of population: universal susceptible • stable and persistent immunity
EPIDEMIOLOGY • 4.Epidemiologic feature: • (1). Season: November - May • high peak: March - April • (2).age: 6 months to 2 years old
PATHOGENESIS • meningococci • extinguished • nasopharynx carriers 60 - 70% • upper respiratory tract • infection 20 -30% • meningococcemia period • septicemia • pyogenic meningitis 1%
Fulminant type endotoxin microcirculatory failure DIC contraction of brain vessel brain edema shock bleeding coma
PATHOLOGY • Septicemic stage: • 1. vascular endothelial injury; • 2. vascular wall inflammation,necrosis, • 3. thrombosis, perivascular bleeding • Meningitis stage: • 1. Site : leptomeninx , arachnoid • 2. congestion, bleeding, swelling of meningeal vessel,
PATHOLOGY • 3. Exudation of fibroprotein , neutrophil and plasma ( CSF is purulent) • 4. cranial nerves is injured. • Fulminant meningoencephlitis type • congestion, bleeding, necrosis and • swelling of brain tissue. • intracranial hypertension • brain hernia
CLINICAL MANIFESTATION • Incubation period: 1~10 days(2~3days) • common type: • 1.URT infectious stage: • 2.septicemic stage: • toxemia symptoms; • petechiae, purpura or ecchymosis. • 3.meningitis stage: • 3.1.High fever and septicemic symptoms;
CLINICAL MANIFESTATION • 3.2.CNS symptoms:headache,vomiting, • meningeal irritation: • nuchal rigidity;Kerning’signs and • Brudzinski’signs are positive. • severe case :drowsiness,delirium, and restless merge into coma. • Convulsions may occur at any stage • of the illness. • 4.Convalescent stage:5~7days from
CLINICAL MANIFESTATION • Fulminant types: 3 forms: • 1.shock form:the most dramatic form; • 1.1.severe toxic symptoms; • 1.2.wildly petechiae, purpura, ecchymosis • 1.3.shock :pallor,extremities cold, cyanosis, hypotension, pales quickly • 1.4.DIC; • 1.5.MOF;
CLINICAL MANIFESTATION • 1.6.Meningeal irritant signs is absent, • CSF is normal; • 1.7.Blood Culture of meningococcus. • 2 . Meningoencephalitis type: • 2 .1.fever,toxic symptoms,petechiae; • 2 .2.repeated convulsions • 2 .3.Intracranial hypertension:
CLINICAL MANIFESTATION • Severe headache;projectile vomiting; • Papillar edema;encephalocele; • respiratory failure. • 3.mixed type: • The mild form: • The chronic meningococcemia form:
Complications • Otitis media,purulent arthritis, • endocarditis,pericarditis,pneumonia or • panophthalmitis. • Sequelae: • hydro-subdura, hydrocephalus, cranial nerves injured,deafness, • blindness,paralysis etc.
DIAGNOSIS • 1.Epidemiologic data: • 2 .Clinical manifestations: • 3 .Lab findings;
Laboratory Findings: • 1.Blood pictures: WBC20x109,PLT is decrease in DIC; • 2.CSF is suppurative; • 3.Bacteriologic diagnosis:smear or • culture; • 4.Immunologic test:antigen and antibody
DIFFERENTIAL DIAGNOSIS • 1.Other purulent meningitis; • 2 .TB MENINGITIS; • 3.Epidemic encephalitis B; • 4.Septicemia.
TREATMENT • COMMON TYPE: • 1.General treatment: • 2 .Pathogenic treatment : • 2 .1.penicillin G: • 2 .2 .Chloramycin: • 2 .3.Ceftriaxone,Cefotaxime; • 3.symptomatic therapy:
FULMINANT TYPE • 1.SHOCK form: • 1.pathogenic therapy; • 2 .Anti-shock; • 3. Steroid;hydrocoticosterone etc; • 4. Anti-DIC; • 5. Protect major organs;
2 .Meningoencephalitis: • 1. Antibiotics; • 2 .Decrease intracranial hypertension; • 3 .Steroid; • 4. Anti-respiratory failure; • 5. Symptomatic treatment;
PREVENTION • 1.Isolation source of infection; • 2.Cut the route of transmission; • 3 .Protect susceptible population: • 3.1.Chemoprophylaxis: • SMZ CO or rifampicin; • 3. 2 .Vaccination.