Download
1 / 40
420 likes | 680 Views
Radiation for Prevention and Treatment of Brain Metastases in Lung Cancer. Minesh Mehta, Northwestern University Chicago, IL. In partnership with . Consultant: Adnexus , Bayer, Merck, Tomotherapy Stock Options: Colby, Pharmacyclics , Procertus , Stemina , Tomotherapy

E N D
Radiation for Prevention and Treatment of Brain Metastases in Lung Cancer Minesh Mehta, Northwestern University Chicago, IL
Consultant: Adnexus, Bayer, Merck, Tomotherapy • Stock Options: Colby, Pharmacyclics, Procertus, Stemina, Tomotherapy • Board of Directors: Pharmacyclics • Data Safety Monitoring Boards: Apogenix • Medical Advisory Boards: Colby, Stemina, Procertus • Speaker: Merck • IP/Patents:Procertus COI Disclosure (2010-11)
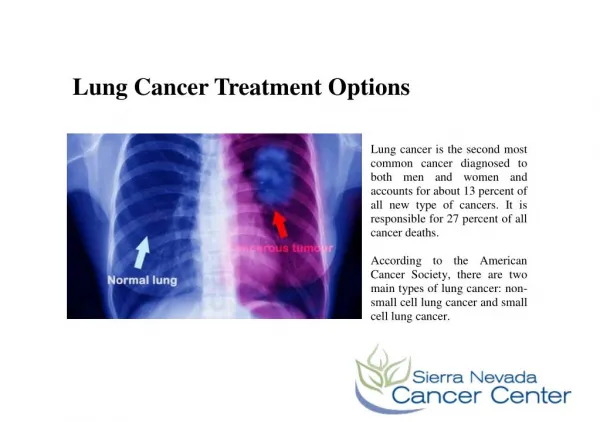
Discuss the role of whole brain radiotherapy in preventing the development of brain metastases in small-cell and non-small cell lung cancer • Discuss the role of radiosurgery in managing brain metastases from NSCLC • Discuss the role of WBRT in conjunction with surgery or SRS Objectives
Although SCLC responds dramatically to chemotherapy, it does not readily penetrate the BBB, resulting in a microscopic sanctuary site. • Intracranial failure rates therefore remain very high • Because of the innate sensitivity of SCLC to XRT, low dose cranial treatment should reduce the likelihood of developing brain mets • Several clinical trials have validated this and a large 1999 meta-analysis showed that PCI reduces the 3-year rate of brain mets by 25% and improves survival by 5% PCI in SCLC
First-Line Chemo-RX: Response of Asymptomatic Brain Metastases From Small-Cell Lung Cancer to Systemic First-Line Chemotherapy* CNS Response Rate: 27% Systemic Response Rate : 73% *Cyt, Adria, & VP16 Tatjana et al., J. Clin Oncol vol 24, pp2079-2083, 2006
Meta-Analysis of Prophylactic Cranial Irradiation Auperin et al, NEJM, 1999 Death Brain Mets • 7 randomized trials, 987 pts with CR; almost all had LS Dz • 5% increase in survival at 3 yrs • Higher dose improved local recurrence but no effect on survival 16% risk 54% risk
PCI in ES-SCLC - Study Design Slotman B et al NEJM: 2007 PCI 20-30 Gy in 5-12 fractions Chemotherapy (4-6 cycles) No response R Any response No PCI < 5 weeks 4-6 weeks Stratification: - Institute - Performance score Primary endpoint – reduction in risk of symptomatic brain mets (HR=0.44)
Symptomatic brain metastases Months from moment of randomization
Slotman JCO, 2009 Hair Loss Global Health Status Role Functioning Fatigue Emotional Functioning Cognitive Functioning Months from moment of randomization
Summary: PCI in ES-SCLC • PCI significantly reduces the risk of symptomatic brain metastases (p<0.001; HR=0.27; 14.6 vs. 40.4% at 1 yr) • No difference in time to extra-cranial progression • PCI significantly prolongs failure-free survival and overall survival (Overall survival: p=0.003; HR=0.68; 27.1 vs. 13.3% at 1 yr) • PCI is well tolerated and does not substantially influence global QoL/health status/cognitive function
A Phase III Comparison of Prophylactic Cranial Irradiation (PCI) versus Observation in Patients with Locally Advanced Non-Small Cell Lung Cancer (LA-NSCLC): QOL and Neurocognitive Analysis RTOG 0214
RTOG 0214: Schema RANDOMIZE STRATIFY PCI 30Gy at 2Gy/Fx No progression after curative therapy for Stage IIIA/B NSCLC* • Stage • IIIA • IIIB • Histology • SCCa • Non-SCCa • Treatment • Surgery • No Surgery OBSERVATION *No CNS metastases by brain MRI or CT
All PCI NSCLC Trials Show Benefit Prospective Randomized Trials of PCI in NSCLC
NCF deterioration occurs early and often. We have analyzed the time course of NCF decline employing 8 prospectively measured domains in 208 brain metastases patients treated with 30 Gy WBRT and have found that: Median time to NCF deterioration was longer in good than in poor responders. Memory was most susceptible to early decline, even in patients with non-progressing brain metastases: the role of the hippocampus Where is the Balance?
Other Strategies • Limit PCI to very high risk populations only • Non-squamous NSCLC patients have 27% risk • Neuroprotectors • RTOG 0614, Memantine • Use BBB-penetrating chemotherapy, e.g. TMZ • SP PO5416, randomized phase II trial • Hippocampal avoidance • To protect the radiosensitive neuro-progenitor stem cell compartment (not anatomic protection)
Median Survival % in Class Class I <65 (age) KPS >70 Controlled primary No extracranial mets 7.1 months 20 Class II – all others 4.2 months 65 Class III – KPS <70 2.3 months 15 WBRT: Survival vs. Class All brain metastases are not equal. Gaspar L, et al. Int J Radiat Oncol Biol Phys. 2000;47:1001-1006. Gaspar L, et al. Int J Radiat Oncol Biol Phys. 1997;37:745-751.
Does Histology Matter?Database Analysis for GPA Sperduto, et al, ASTRO 2010
Does Histology Matter?Database Analysis for GPA Sperduto, et al, ASTRO 2010
Regression of brain mets after WBRT correlates with survival and improved neurocognitive function
WBRT + MGd Response Analysis Volume reduction > 45% Good responders 135 pts at 2 mo Poor responders Median tumor volume reduction at 2 mo: 45% Volume reduction < 45%
Tumor Shrinkage Prolonged Survival Response MS Good 300+26 d Poor 240+19 d P-value 0.03
100 RT + RS (MS=6.5 mos) RT alone (MS=4.9 mos) 80 P=0.0470 60 % Alive 40 Survival of Pts with 1 Brain Met 20 0 0 6 12 18 24 Months Andrews DW, et al. Lancet 2004;363:1665-1672.
Bhatnagar et al., IJROBP, 2006. Retrospective study: 205 patients with various malignancies Radiosurgery for 4 or more metastases. Median marginal dose of 16 Gy. Median overall survival was 8 months. RPA classes I, II, and III: 18, 9, and 3 months Tumor volume was the most significant predictor of survival and the only significant predictor of local control; number of lesions was not a significant prognostic factor. Radiosurgery for Multiple Mets
Very High Brain Relapse After Surgery if WBRT is Omitted Complete resection without WBRT leads to 70% actuarial relapse This is a relative risk of 3 Patchell, JAMA.1998:280:1485
82 pts on JROSG 99-1 had MMSE 27 Median time to 3 point drop: 16.5 vs. 7.6 months, in favor of WBRT+SRS (p = .05) 12 and 24 month freedom from 3 point drop: 76 and 69% for WBRT+SRS vs. 59 and 52% for SRS alone Progressive disease is worse than WBRT Impact of WBRT on MMSE Aoyama, Int J Radiat Oncol Biol Phys, 68:1388-395, 2007
Roles of WBRT for NSCLC Brain Mets Preventative SCLC NSCLC Therapeutic Multiple Brain Mets Adjunctive To reduce local failure after SRS/S To reduce regional failure after SRS/S Toxicities MMSE changes are minor to none and might even improve Finer tools pick up some decline, mostly early, with some late recovery Conclusions