Download
1 / 31
310 likes | 550 Views
DCIS – Are we cutting it?. Dr Alex Lemaigre With thanks to: Mr Richard Boulton Dr Elizabeth Osinibi Mr Oladapo Fafemi. Introduction to DCIS. Ductal carcinoma in situ Non invasive neoplasm in the milk ducts of the breast Predisposes to invasive ductal carcinoma

E N D
DCIS – Are we cutting it? Dr Alex Lemaigre With thanks to: Mr Richard Boulton Dr Elizabeth Osinibi Mr OladapoFafemi
Introduction to DCIS • Ductal carcinoma in situ • Non invasive neoplasm in the milk ducts of the breast • Predisposes to invasive ductal carcinoma • 2900 cases of screen-detected DCIS per annum (9)
DCIS - Treatment • Usually wide local excision (lumpectomy) +- radiotherapy. • Prognosis improved by greater resection margin, and the use of radiotherapy.(1,2,3) • Sentinel node biopsy (SNLB) not recommended (incidence LN metastases <1%). (4,5)
Aims and Objectives • To discover how many of DCIS cases on core biopsy will be found to have invasive cancer on excision histology. • Can we predict which these will be? • Should we be doing SNLB on these patients? • How successful are we at adequately excising the neoplasm with wide local excision?
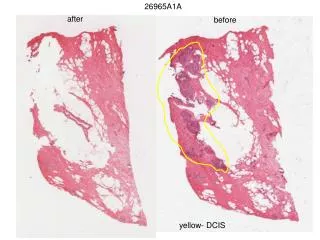
Methods • Analysed all new patients diagnosed with DCIS only on core biopsy in 2009, 2010 and 2011. • grade of initial DCIS • diagnosis on excision specimen • closest resection margin • need for re-excision
Inclusion criteria: all patients newly diagnosed with DCIS ONLY on core biopsy in 2009, 2010 or 2011, regardless of age, sex, or method of detection. • Exclusion criteria: Recurrent breast cancer, DCIS + any other diagnosis on core biopsy. • Where multiple grades of DCIS were present in a specimen, the highest grade was considered.
Results • Total 36 patients with DCIS only in 3 years
Conclusions • 19% of patients with DCIS only on core biopsy were found to have invasive ductal carcinoma on excision histology. • These patients cannot be predicted by the initial grade of the DCIS. • High grade DCIS does not increase the risk of invasive cancer compared to lower grades.
Resection Margins • Analysed the resection margins on excision specimens. • 1 case was excluded as the patient had a mastectomy for multifocal DCIS • 1 case was excluded as the biopsy appeared to have entirely excised the DCIS • Total = 34 patients
North Middlesex standard “safe” excision margin for DCIS = 5mm • There is some variability between centres on this figure (1mm – 10mm).
NB – total number here = 45 as many specimens had >1 margin reported as close
Need for Re-excision? • According to these data 11 out of 34 cases had wide enough resection margins. • Therefore 23/34 (67%) require re-excision to improve margins. • However – improving the posterior margin involves resecting the chest wall (including pectoralis major). • There is no prognostic benefit to this, and it causes greater morbidity. • Excluded those where the posterior margin was the only close margin <5mm (n=3)
The Saga Continues... • 20 cases still require re-excision • = 55% of our original population of 36 patients • 2 had a mastectomy • 1 was referred to Royal Free • 2 lost to NMUH follow-up • 11 had successful re-excision • 4 had inadequate re-excision
Conclusions • 55% of DCIS patients required more than one operation to adequately clear the DCIS
Discussion – Excision histology + SLNB • SLNB used in invasive cancer to determine lymph node spread. • SLNB cannot be performed after WLE due to disruption of lymphatic drainage. • DCIS grade does not predict probability of invasive carcinoma. • Therefore cannot guide us which patients to select for SLNB. • No value in SLNB on DCIS patients as <1% will show LN involvement (4,5).
Ductal carcinoma in situ • 1.4.5 Do not perform SLNB routinely in patients with a preoperative diagnosis of DCIS who are having breast conserving surgery, unless they are considered to be at a high risk of invasive disease. • 1.4.6 Offer SLNB to all patients who are having a mastectomy for DCIS.
Discussion – Excision Margins • Surgery for DCIS aims to balance disease clearance (and risk of recurrence) and an acceptable cosmetic appearance. • No prospective trials have assessed optimum excision width for in situ disease. • Involved margins carry the worst prognosis (6) • No consensus on standard acceptable margins • How do we decide?
1.3 Surgery to the breast • Ductal carcinoma in situ • 1.3.1 For all patients treated with breast conserving surgery for DCIS a minimum of 2 mm radial marginof excision is recommended with pathological examination to NHSBSP reporting standards. Re-excision should be considered if the margin is less than 2 mm, after discussion of the risks and benefits with the patient. • 1.3.2 Enter patients with screen-detected DCIS into the Sloane Project (UK DCIS audit)[5]. • 1.3.3 All breast units should audit their recurrence rates after treatment for DCIS.
Discussion – Re-excision rates • 55% re-excision seems very high. • Wong et al stated a re-excision rate of 84% to achieve margins of >10mm. (7) • Holland et al stated a re-excision rate of 43% to achieve margins of >1mm. (8) • Re-excision rates will depend on what distance the excision margin is considered safe.
Discussion - Radiotherapy • Post-operative radiotherapy significantly decreases risk of disease recurrence (1,2,3). • Julien et al 2000: 4 year recurrence free = 84% vs 91% if treated with radiotherapy (1) • Chan et al 2001: Recurrence of 18.6% vs 11.1% if treated with radiotherapy (3) • Wong et al 2006: abandoned trial of WLE only (10mm margin) due to high recurrence rate of 2.4% per patient year. (7) • NMUH does not routinely offer radiotherapy to DCIS patients
1.11 Radiotherapy • Radiotherapy after breast conserving surgery • 1.11.1 Patients with early invasive breast cancer who have had breast conserving surgery with clear margins should have breast radiotherapy. • 1.11.2 Offer adjuvant radiotherapy to patients with DCIS following adequate breast conserving surgery and discuss with them the potential benefits and risks (see recommendation in section 1.3.1)
Further Work • Audit recurrence rates in these patients. • Compare our results with rates of re-excision data from other centres with similar choice of acceptable margins. • Compare our data with previous data collected by Mr Fafemi some years ago.
References • Julien J, Bijker et al. Radiotherapy in breast conserving treatment for ductal carcinoma in situ: first results of EORTC randomized phase III trial 10853. Lancet 2000; 355:528-33. • Fisher ER, Dignam J et al. Pathologic findings from the National Surgical Adjucant Breast Project (NSABP) eight-year update of Protocol B-17 intraductal carcinoma. Cancer 1999;86:429-38 • Chan KC, Knox WF et al. Extent of excision margin width required in breast conserving surgery for ductal carcinoma in situ. Cancer 2001;91:9-16 • Kitchen PR, Cawson JN et al. Axillary dissection and ductal carcinoma in situ of the breast: a change in practice. Aust NZ J Surg 2000;70:419-22 • Veronesi P, Intra M et al. Is sentinel node biopsy necessary in conservatively treated DCIS? Ann Surg Oncol 2007;14(8):2202-8 • Law, Tsz Ting MBBS; Kwong, Ava FRCS. Surgical Margins in Breast Conservation Therapy: How Much Should We Excise? Southern Medical Journal: December 2009 - Volume 102 - Issue 12 - pp 1234-1237 • Wong J, Kaelin CM et al. Prospective study of wide local excision alone for ductal carcinoma in situ of the breast. J clin oncol 2008;24(7):1031-1036 • Holland PA, Gandi A, et al. The importance of complete excision in the prevention of local recurrence of ductal carcinoma in situ. Br J Cancer 1998; 77(1):110-114. • Dodwell D, Clements K, Lawrence G, Kearins O, Thomson C, Dewar J, Bishop H, on behalf of the Sloane Project Steering Group. Radiotherapy following breast-conserving surgery for screen-detected ductal carcinoma in situ: indications and utilisation in the UK. Interim findings from the Sloane Project. British Journal of Cancer 2007; 97: 725-729 • NICE guidelines – Feb 2009 – Early and locally advanced breast cancer, diagnosis and treatement.