Download
1 / 30
300 likes | 350 Views
This resource explores the critical role of Human Resources (HR) in health systems and the challenges faced during decentralization efforts, such as poor staff motivation, problems with incentives, and staffing distribution issues. Key topics addressed include new skills and job descriptions, incentives, overstaffing, separation from civil service, and managing conflicts. The text delves into the shifts needed in organizational structures and HR practices for successful decentralization in health care.

E N D
Human resources (HR) take up the major part of the health system’s budget and play a significant role in the amount and quality of health care provision. • Paradoxically, they have not been a key part of the health sector reforms introduced in many countries.
Problems of health human resources in developing countries. • Poor staff motivation • Lack of clear incentives • Inequitable distribution of staff • Instability in staffing • Recruitment of poorly trained staff • Non-existent supervision
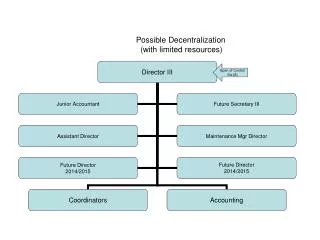
HR and Decentralization • Decentralization calls for changes in the way human resources are organized into functional health care structures and in the jobs that staff perform. • Organizational structures and positions at both the central and local levels require modification to conform with the new division of powers and resource allocation patterns. • Shaping the post-decentralization pattern of employment in the health sector through organizational design and job re-profiling is highly complex on a technical and operational level.
Key Issues of Human Resources in Decentralization • New Skills and Job Descriptions • Incentive Structures • Hiring, firing and transfers • Overstaffing • Separation from Civil Service • Pension Responsibilities • Health Professionals vs. Local Authorities • Recruitment and Distribution • Training and Education • Managing Conflict
New Skills and Job Descriptions • Define new tasks and skill needs based on institutional assessment • Redefine job descriptions for appropriate tasks and skills • Avoid overlap and uncertainty of tasks and responsibilities • Training in new skills • Recruitment of new staff
Incentives in large organizations • Monetary • Salary scale – tends to reward longevity more than skills and performance • Benefits – pensions, insurance • Bonus – can be tied to performance • Non-monetary • Housing, schooling, other benefits • Promotion opportunities • Training opportunities • Symbolic rewards
Incentives -Problems • Problem of declining budgets and increasing percentage allotted to salaries • Problem of competition with private sector for providers and effect on salaries and hours • Do local authorities have control over incentives for health workers? • Can they use non-monetary incentives? • Problem of Incentives for Rural Service • Restrictions of Labor Laws and Civil Service
Hiring and Recruitment • Avoiding patronage and creating merit hiring process • Appropriate pre service training requirements • The role of Civil Service regulations • Permanent vs. Contract staffing • Current skill level in national or local labor pool
Problem of Overstaffing • Determining the extent of overstaffing • Approaches for reducing staff • Golden Handshake • Exit training
Separation from Civil Service • Devolution often accompanied with change in employment status for health staff • Usually means reduction in protections and increased local capacity to hire and fire • Shift from national civil service protection to: • local municipal civil service • general private sector labor laws
Separation from Civil Service • Loss of career path from primary to higher levels of care and administration • Usually loss of civil service protection is the major issue of opposition to devolution by health workers
Pension Funding • Pensions for health workers usually funded in pay-as-you-go plan with no separate fund • In devolved systems, local authorities refuse to accept responsibility for pensions of prior civil service staff • Usually need to create new fund to cover pensions and transfer control of funds to local authorities
Health Staff vs. Local Authorities • Education and status differences • Differing priorities • Local health staff as advocate for Ministry priorities
Planning, Distribution and Recruitment • Poor areas are at disadvantage in attracting staff and urban wealthy areas have surpluses • Centralized planning and assignments may improve distribution of staff in unattractive areas • Centralized planning and assignment may not overcome problem but decentralized recruitment may make it worse
Training and Education • Economies of scale and quality control in centralized training programs • Decentralization of responsibility for training may weaken training capacities at poorer localities • Failure to define roles and responsibilities and to assign sufficient funding during transition
Managing Conflict • Transparency of recruitment, promotion, and disciplinary processes • Role of unions • Politicization of labor conflicts is often the problem of health officials at all levels
When are localities ready? • Lack of appropriate human resources is often used as justification for centralization • Can we wait until appropriate staff is in place? • Role of “demand for skills” in recruitment and training
Decentralization and Human Resource: Main Issues and Problems HR planning and staff supply HRD planning and decentralization Lack of synchronization between decentralization and HRD policies Staff needs assessment Lack of staff need assessment for decentralized units to address issues on equity and work load Employment pattern Shift to employing more temporary and short term or contract based staff; De-linking of health personnel from civil service; Transfer of staff from Ministry of Health to local authority, Contracting out supportive services Staff mix Changing staff mix and impact on costs and types of care Recruitment, retaining and re- deploying existing health personnel Inequitable staff distribution between decentralized areas; Role of central transfers in allocating staff to disadvantaged areas; The effects of nepotism on local recruitment Personnel administration and employee relations Authority over staff Mixture of local and central control over different aspects of staff management Staff pay/salary Strong central control remains in some cases; Limited local capacity for setting up local pay scheme; Pay inequality created between decentralized areas
Decentralization and Human Resource: Main Issues and Problems Performance management Supervision Poorly defined supervision system; Reduced logistics for conducting supervision tasks; Lack of technical supervision capacity Performance appraisal Lack of resource at periphery affecting performance; Lack of local capacity for performance appraisal; Lack of clear job description; Resistance to performance related pay by staff Education and Training Reduced resources for staff training at local level Managing change Capacity strengthening Mixture of local and central control over different aspects of staff management Power relations and conflict Conflicts between different professional and managerial Groups; Reduced staff motivation Change process Inadequte communication and dialogue between reformer and health personnel
Thank You! Any Question?
Questions to Answer about HR & Decentralization • How will the future roles of central and local staff be defined? • How will future planning decisions on the number and type of staff that the nation should develop be made? • How and by whom will decisions on the staff strength of each decentralized administrative entity be made? • How will personnel information be gathered and data bases maintained? • How will salaries be set and paid for? • Is this arrangement financially viable in the long term? • What will happen to pensions and other benefits? • Will established career structures be maintained?
Questions to Answer about HR & Decentralization • Will in-service and continuing training opportunities at the decentralized level be sufficient to ensure career development? • How will staff performance be assessed and by whom? • Who will be responsible for hiring and firing at the local level? • What mechanisms will be put in place to address personnel grievances? • What will be the procedures for transferring health staff from one authority to another? • What will be the new roles and responsibilities of training institutions? • What legal implications will decentralization have for the duties and rights of health workers?
Second, the definition of personnel management processes after decentralization must proceed in parallel with the design of organizational structures. • Decisions on how salary scales and position levels are decided, and how recruitment, selection, appointment, performance assessment, or staff discipline will be handled are complex, time-consuming, and again, subject to the influence of a central civil service agency.
Third, existing staff members must be reallocated to new organizational structures. • Personal preferences, career ambitions, or fear of change can make the process of staff allocation an area of high anxiety and much discord. • If skilled managers are few, the central-level staff may feel particularly uncomfortable in their proposed new roles as experts and technical advisors and oppose any change. • In Papua New Guinea, for example, central-level technical officers who were not well qualified for a role of an expert advisor at the time of decentralization vigorously resisted revising the organizational structure.
Fourth, the personnel files of decentralized health workers must be transmitted to the management level that is now responsible for them. • Compiling an accurate personnel record for each individual, with available data on their qualifications and training, employment, salary history, and record of performance, together with the physical transfer of these records, can be a mammoth task. • In Mexico, for example, devolution of health services involved the transfer of 116,000 health workers to the state governments.
Fifth, mechanisms are required to mediate disputes regarding the transfer of human resources that may arise between the central and local levels. • Chief officials at the decentralized management level may, for legitimate reasons of efficiency or resource constraint, refuse to accept a particular post into their organizational structure. • In the Philippines, local chief executives were unwilling to absorb over 4 per cent of the Department of Health personnel by the time the full transfer of assets to local government units (LGUs) was to have been completed.
Finally, managers must decide how to deal with health workers who will not or cannot transfer to their new jobs. • These health workers may object to a physical relocation that their reassignment to a new organizational structure demands because of family problems or a lack of accommodation in the new locale.
Staff transfers are particularly opposed, when workers are concerned about the long-term security of their employment.
The impact of professional associations, unions and registration bodies • Health workers’ associations, unions, and registration bodies are a very powerful force in the design and implementation of decentralized management structures and jobs. • A common fear of the members of health workers’ associations and unions is that decentralization will jeopardize their tenure or substantially reduce their salaries and benefits. • In South Africa, the employment of local government can earn 40 to 70 percent more than the provincial health departments