Download
1 / 52
560 likes | 968 Views
From Guidelines to Bedside: Clinical Case Scenario Approach. Mazen Kherallah, MD, FCCP. Treatment of Invasive Candidiasis in ICU. Risk Factors. Markers. Signs & symptoms. Full blown disease. Clinical. Prophylaxis. Pre-emptive. Empiric. Directed. Treatment. 41. 40. 39.

E N D
From Guidelines to Bedside: Clinical Case Scenario Approach Mazen Kherallah, MD, FCCP
Treatment of Invasive Candidiasis in ICU Risk Factors Markers Signs & symptoms Full blown disease Clinical Prophylaxis Pre-emptive Empiric Directed Treatment 41 40 39 Temperature (°C) 38 37 36 Anti Mannan + + (1.3)-Beta-D-glucan Disease likelihood Remote Probable Possible disease Proven
Overall Mortalityin Patients with Invasive Candida Infections
Mortalityper Candida Species Horn DL, Neofytos D, Anaissie EJ, Fishman JA, Steinbach WJ, Olyaei AJ, et al: Epidemiology and outcomes of candidemia in 2019 patients: data from the prospective antifungal therapy alliance registry. Clin Infect Dis 2009,48:1695-1703.
Delaying the Empiric Treatment of Candida Bloodstream Infection until Positive Blood Culture Results Are Obtained: a Potential Risk Factor for Hospital Mortality Morrell M, Fraser VJ, KollefMH, Antimicrob Agents Chemother 2005; 49:3640–5.
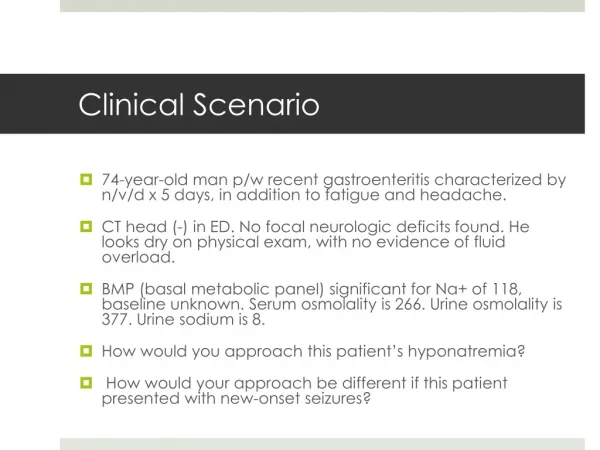
Case Study #1 • 39-year-old black man with DM who was admitted 8 days ago for complications of end-stage liver disease, including acute renal failure and ascites, he also had diffuse lymphadenopathy of unknown etiology. • A week before hospitalization, the patient had been discharged from another hospital, where he had been admitted because of pancreatitis and treated for Escherichia coli bacteremia and renal insufficiency.
Case Study #1 (cont’d) • On day 8, 1 out of 4 bottles of blood cultures was reported positive for yeast. • Patient’s clinical status had deteriorated because of worsening respiratory distress.
What is the likelihood that this yeast would be candida non-albicans in your unit? • 10% • 25% • 50% • 75% • We have no data
Epidemiology: Spain (1994–2008) M. Ortega et al: J Antimicrob Chemother 2010; 65: 562–568
Epidemiology: IRAN (2005–2010) BadieeP, Alborzi A: IRAN. J. MICROBIOL. 3 (4) : 183-188
How would you approach the patient? • Repeat blood cultures and observe • Fluconazole • Caspofungin • Lipid Formulation Amphotericin B
Treatment of Invasive Candidiasis in ICU Risk Factors Markers Signs & symptoms Full blown disease Clinical Prophylaxis Pre-emptive Empiric Directed Treatment 41 40 39 Temperature (°C) 38 37 36 Anti Mannan + + (1.3)-Beta-D-glucan Disease likelihood Remote Probable Possible disease Proven
Recent Exposure to Caspofungin or Fluconazole Influences theEpidemiology of Candidemia: a Prospective MulticenterStudy Involving 2,441 Patients Fluconasole Caspofungin Proportion of the five major Candida species responsible for fungemia in patients with (n 159) or without (n 2,289) prior exposure to fluconazole (P 0.001) or with (n 61) or without (n 2,387) prior exposure to caspofungin(P 0.001): Olivier Lortholary et al. ANTIMICROBIAL AGENTS AND HEMOTHERAPY, Feb. 2011, p. 532–538
HachemRet al: The changing epidemiology of invasive candidiasis: Candida glabrataand Candida kruseias the leading causes of candidemia in hematologic malignancy. Cancer 2008, 112:2493-2499. Cohen Y et al. Early prediction of Candida glabratafungemia in nonneutropenic critically ill patients. Crit Care Med 2010, 38:826-830. Wey SBet al: Risk factors for hospitalacquiredcandidemia. A matched case–control study. Arch Intern Med 1989, 149:2349-2353.
Candidemia: non-neutropenicFluconazole (loading dose of 800 mg [12 mg/kg], then 400 mg [6 mg/kg] daily) or an echinocandin(caspofungin: loading dose of 70 mg, then 50 mg daily; micafungin: 100 mg daily; anidulafungin: loading dose of 200 mg, then 100 mg daily) is recommended as initial therapy for most adult patients (A-I) Caspofungin 2008 IDSA Candidiasis Guidelines Treatment Guidelines for Candidiasis • CID 2009:48 (1 March) • 505
Case Study #2 • 65 year old patient in the ICU after hemicolectomy for perforated cecal diverticulitis who was treated with pip/taz and fluconazole and has been on ventilator for the past 12 days • Course was complicated with VAP but sputum culture showed mixed organisms with candida sp.
Case Study #2 (cont’d) • Now with fever to 39.0 as well as hypotension (70/40 mm Hg) and tachycardia (120/,im). • Physical examination is remarkable for toxic-appearing man who is orotracheally intubated and sedated. • He has a triple lumen central venous catheter at the right subclavian vein site that was inserted 10 days ago for TPN • The skin is mildly erythematous around the catheter site, but no tenderness or drainage
Case Study #2 (cont’d) • Serum creatinine 140 mmol/L, WBC 14,500, 90% Neutrophils with toxic granulation • There is no clinical or radiographic evidence of pneumonia, sinusitis or other source of infection. • Treated with imipenem and vancomycin after removing the line but no improvement for the past 2 days
How would you approach this case? • Repeat cultures and continue same antimicrobial agents with close observation • Add colistin to current antimicrobial agents • Add colistin and fluconazole at 400 mg IV daily • Add colistin and caspofungin at 70 mg initial dose then 50 mg daily
Promoting Colonization Alteration of Natural Host Barriers Host Factors Organism Anti Mannan (1.3)-Beta-D-glucan
Patients at Risk for Invasive Candidiasis Colonization Index Candida Score Predictive Rule N◦sites +/N◦ site screened 2X weekly > 0.5 or ≥ 0.4 corrected • Surgery on ICU admission • TPN • Severe sepsis • Candida colonization • >2.5 points ≥ 4th day of ICU stay: Sepsis+CVC+MV+1 of: TPN (day 1-3) HD (day 1-3) Major surgery (within 7 days) Pancreatitis (within 7 days) Immunosuppression or steroids (within 7 days) Start Empirical Antifungal Therapy Patients treated: 10-15% Candidiasis captured: 85-90% Patients treated: 15-20% Candidiasis captured: 75-85% Patients treated: 10-15% Candidiasis captured: 60-75%
Performances of (1®3)-b-D-glucan assay (BG), Candida score (CS), and colonization index for detection ofinvasive candidiasis in 95 patients Posteraro et al. Critical Care 2011, 15:R249
Treatment of Invasive Candidiasis in ICU Risk Factors Markers Signs & symptoms Full blown disease Clinical Prophylaxis Pre-emptive Empiric Directed Treatment 41 40 39 Temperature (°C) 38 37 36 Anti Mannan + + (1.3)-Beta-D-glucan Disease likelihood Remote Probable Possible disease Proven
Case Study #3 • 29 year old male with no significant past medical history who was admitted to the hospital 4 days ago after he suffered multiple injuries secondary to road traffic accident: • Left multiple rib fractures with pulmonary contusion and hemothorax, required left chest tube drainage and mechanical ventilation
Case Study #3 • Splenic rupture with intra-abdominal bleed required splenectomy • Intestinal injury that required resection and anastomosis • Patient started on TPN through left sided subclavian central venous line Empiric antibiotic with piperacillin/tazobactam was started on day #1
What would you do next? Day #4: Patient is has no fever or leukocytosis, how would you approach his antibiotic regimen: • Continue piperacillin/tazobactam for total of 10 days • Change to Imipenem/cilastatin • Add flucanozole • Add Caspofungin • Stop antibiotics and observe
Treatment of Invasive Candidiasis in ICU Risk Factors Markers Signs & symptoms Full blown disease Clinical Prophylaxis Pre-emptive Empiric Directed Treatment 41 40 39 Temperature (°C) 38 37 36 Anti Mannan + + (1.3)-Beta-D-glucan Disease likelihood Remote Probable Possible disease Proven
Fluconazole Prophylaxis Prevents Intra-abdominal Candidiasis in High-risk Surgical Patients Eggimann P., Crit Care Med 1999, 27:1066-1070
Antifungal agents for preventing fungal infections in non-neutropenic critically ill and surgical patients: Invasive Infections E. G Playford et al Journal of Antimicrobial Chemotherapy (2006) 57, 628–638
Antifungal agents for preventing fungal infections in non-neutropenic critically ill and surgical patients: Mortality E. G Playford et al Journal of Antimicrobial Chemotherapy (2006) 57, 628–638
Risk-based fluconazole prophylaxis of Candida bloodstream infection in a medical intensive care unit Faiz et al: Eur J Clin Microbiol Infect Dis (2009) 28:689–692
Risk-based fluconazole prophylaxis of Candida bloodstream infection in a medical intensive care unit Only 2.6%of patients met the rule and were administered prophylaxis, Faiz et al: Eur J Clin Microbiol Infect Dis (2009) 28:689–692
Randomized Study of Caspofungin Prophylaxis Followed by Pre-emptive Therapy for Invasive Candidiasis in the Intensive Care Unit • Patients were hospitalized for at least 3 days, ventilated, received antibiotics, had a central venous catheter at any time in the first 3 days • +1 of the following: • Major surgery • Parenteral nutrition or dialysis • Pancreatitis • Systemic steroids • Other immunosuppressive agents within 7 days prior to or on ICU admission Subjects were followed daily for IC. (1,3)-b-D-glucan (BG) levels were monitored 2x/week. The primary endpoint was incidence of proven or probable IC by EORTC/MSG criteria. MSG-01,www.clinicaltrials.gov, SHEA 2011 Texas (Society for Healthcare Epidemiology of America)
Randomized Study of Caspofungin Prophylaxis Followed by Pre-emptive Therapy for Invasive Candidiasis in the Intensive Care Unit DRC: data review committee IC: Invasive Candidiasis. MSG-01,www.clinicaltrials.gov, SHEA 2011 Texas (Society for Healthcare Epidemiology of America)
Case #4 • 67 year old female with history of COPD and CVA. • Admitted with COPD exacerbation and has been dependent on the ventilator for the past 2 weeks • Developed VAP and sputum culture revealed C. albicans, treated with Imipenem and vancomycin • Chest x-ray did not improve, BAL was done and confirmed the growth of c. albicans
How would you approach the patient? • Observation • Fluconazole • Caspofungin • Lipid Formulation Amphotericin B
Candida species isolated from respiratory secretions?Growth of Candida from respiratory secretions rarely indicates invasive candidiasis and should not be treated with antifungal therapy (A-III) 2008 IDSA Candidiasis Guidelines Treatment Guidelines for Candidiasis • CID 2009:48 (1 March) • 505
Case #5 Your patient with candidemia who has been started on caspofunginis stable on mechanical ventilation. He is sedated and MAAS score is 0-1, his WBC is decreasing and he has low grade fever. • Your next step is: • Observation • Change to Fluconazole • Ophthalmic examination • Change to Ampho B
Candida Endophthalmitis • All patients with candidemia should have at least 1 dilated retinal examination early in the course of therapy(A-II). • Especially in patients who cannot communicate regarding visual disturbances. • AmB-d combined with flucytosine(A-III) • Fluconazole is an acceptable alternative for less severe cases (BIII). • LFAmB, voriconazole, or an echinocandinfor intolerant or treatment failure (B-III) • At least 4–6 weeks (A-III).
Case #6 • 74 year old male who has been in the intensive care unit for the past 8 days intubated on mechanical ventilation for acute CVA. • His urinalysis showed 10-15 WBC and urine culture grew C. albicans • Foley catheter is in place
How would you approach the patient? • Observation • Change Foley catheter and observe • Fluconazole • Caspofungin • Amphoterecin B bladder irrigation
Urinary tract infections due to Candida species? • Asymptomatic: • Treatment is not recommended unless the patient belongs to a group at high risk of dissemination (A-III). • Elimination of predisposing factors often results in resolution of candiduria(A-III). • High-risk patients include neutropenic patients, infants with low birth weight, and patients who will undergo urologic manipulations. • Symptomatic Cystitis/Pyelonephritis • Fuconazole • AmB-d