Download

1 / 108
1.13k likes | 1.71k Views
From Pain to Comfort. Meg Beturne MSN,RN,CPAN,CAPA. Objectives. Define pain Discuss pain assessment and management utilizing ASPAN’s Clinical Practice Guideline Identify pharmacological and non-pharmacological interventions Describe the challenge of chronic pain in perioperative areas

E N D
From Pain to Comfort Meg Beturne MSN,RN,CPAN,CAPA
Objectives • Define pain • Discuss pain assessment and management utilizing ASPAN’s Clinical Practice Guideline • Identify pharmacological and non-pharmacological interventions • Describe the challenge of chronic pain in perioperative areas • Discuss comfort management
PAIN DEFINED • Pain is usually a localized physical suffering associated with bodily disorder • Pain is one of the body’s most important protective mechanisms • Pain is a complex mechanism with unpleasant physical, emotional and cognitive components associated with actual or potential tissue damage
Pain: The Sixth Vital Sign • Pain is “whatever the person experiencing it says it is, and existing whenever the person says it does”- Gold Standard • The patient is the ONLY one who can accurately describe his/her pain • It is subjective • All pain should be considered REAL • Pain can negatively affect the body McCafferty,2011
Newest Insights • Definition of Pain refined: • Person’s inability to verbally communicate does not preclude the possibility that pain is present • Does not negate the responsibility of healthcare providers to treat it!
Case Scenario • Example: 30 year old female SBO first day post-op; tells you she is in pain & is on phone talking. Do you still believe her? • YES! Pain is subjective and she is using distraction successfully which is a non-pharmacological way to manage pain • Since it is distracting her from the pain, you can now medicate her appropriately
Pain Pathways • Nociceptors: give the body the ability to produce pain • Nerve endings present in skin, viscera, blood vessels, muscle, joints • Activated by noxious stimuli, leads to inflammation & release of bradykinin & prostaglandins • Pain impulses initiated by direct tissue damage and by release of chemicals • Pain travels very fast!
Pain Conduction • Transduction: cutaneous nociceptors send impulses to spinal cord • Transmission: Impulses synapse either by fast or slow pain fibers • Perception: pain impulses processed by thalmus & cerebral cortex • Modulation: along the efferent fibers, pain may be inhibited or modulated
Pain Threshold & Tolerance • Threshold: point at which stimulus is perceived as painful; fairly uniform person to person • Tolerance: maximum intensity of duration of pain a person is willing to endure before needing some intervention; this varies from person to person • Tolerance is not to be judged as acceptable or unacceptable by health care providers
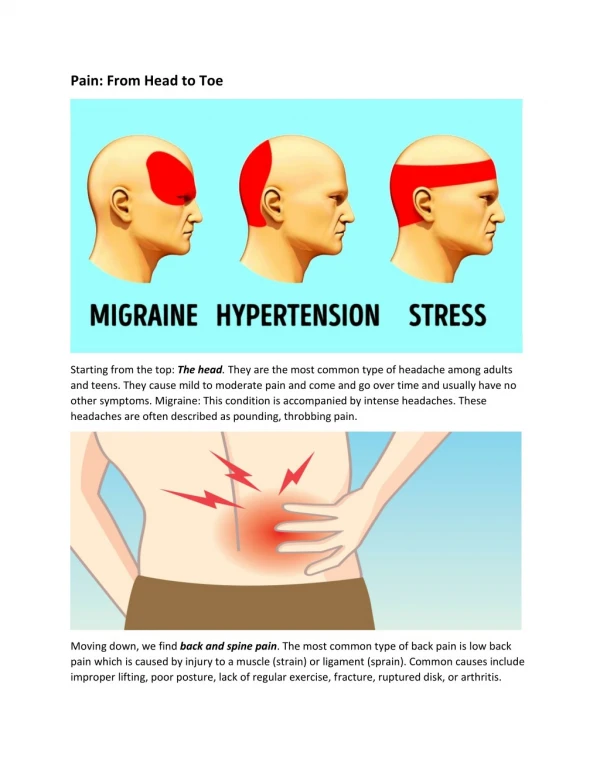
TYPES • Cutaneous: arises from superficial structures ( skin and subcutaneous areas) • Sharp, cutting, burning, throbbing, localized • Burn or paper cut • Deep Somatic: originates in deep body structures ( muscles, bones, tendons, joints) • Characterized as dull or diffuse • Muscle cramps
MORE TYPES • Visceral: origin is in visceral organs • Deep, dull, poorly localized • Associated with nausea & vomiting, hypotension, weakness • Referred: perceived at a site different from its point of origin • Chest pain ( cardiac muscle doesn’t have pain receptors); pain can move to left arm, jaw • Gallbladder pain felt in the shoulder
ACUTE PAIN • Acute: pain that extends until period of healing (less than 6 months), “temporary” • Identifiable cause • Occurs soon after injury • Onset sudden or slow • Intensity mild to severe • Autonomic response: BP,RR,HR increased; pupils dilated; diaphoresis, pallor, facial grimacing, restlessness, guarding behavior
CHRONIC PAIN • Chronic: extends beyond (3-6 months) • May limit ADLs • May not have identifiable cause • Non protective ( serves no purpose) • May lead to depression, fatigue, insomnia, anorexia, apathy & learned helplessness • Autonomic response: BP,HR, RR, Pupils, skin are all normal • If severe & prolonged, PNS activated= muscle tension, HR & BP low, failure of body’s defenses
Point of Emphasis • Physiological signs ( i. e. elevated blood pressure and elevated heart rate) are least sensitive indicators of pain, especially in chronic pain • Don’t withhold pain medication because of these changes alone
CHRONIC- Two Types • Chronic Non-Malignant • Ongoing, lasting more than 6 months • NOT due to life threatening causes • NOT responding to currently available treatments • May continue for remainder of life • Low back pain, arthritis, neuralgia, Crohn's, migraines, peripheral neuropathy • Chronic Malignant • Cancer pain
Chronic Pain in the Sexes • Conditions associated with chronic pain in women: Fibromyalgia, IBS, Rheumatoid Arthritis, Migraines; possible hormonal links; focus on emotional aspects; more likely to seek help than males; helpful to re-label pain as being manageable • Conditions associated with chronic pain in men: cluster headaches, gout, heart disease; focus on sensory aspects
Chronic Pain, Surgical Patient • Require special consideration & planning for pain management :Methadone, Suboxone • Request consultation with acute pain service, anesthesia consultation • Continually communicated individualized pain management plan • Add, optimize first-line meds; rotate opioids • Educate patient to bring in chronic pain medications ( migraine, back pain) • Patient role in goal setting
Other PAIN Terms • Breakthrough Pain: pain that increases above the pain addressed by the ongoing analgesics • Neuropathic Pain (Pathologic): arises from nervous system (peripheral or CNS)- has multiple mechanisms- shooting, sharp, electric • Discomfort: being uncomfortable in body or mind; mild distress • Suffering: feel pain/distress; sustain harm; injury, pain or death
Sobering Statistics • 15% Americans with major trauma/surgery pain (45 million) • 25% Adults have chronic pain ( > 76 million) > diabetes, heart disease, cancer combined • 50% of inpatients/outpatients have pain • 30% patients give hospital low marks for pain control • Untreated/undertreated pain still common CDC (2007) Fast Facts
The Truth About PAIN • Lack of expression does not equal lack of pain~ physiologic and behavioral adaptations to pain occur • Not ALL causes of pain are identifiable • Respiratory tolerance is rapid • Sleep is possible with pain but not good quality • Elderly experience pain but do not express it as much and so do babies! • Addiction is rare 0.1-0.3%
Pain: A Perioperative Problem • Nearly all patients have postoperative pain 45million: 80% rate it moderate to severe • Pain is the most common reason for elective procedures • Fear of pain is the #1 reason for delaying elective surgery: reported by 59% pts. • 50% patients still have pain 1 year after surgery; 30% still have pain 10 years later! National Center Health Statistics,2006
Patient Expectations • If pain is present: • A professional, comprehensive assessment • Individualized evaluation methods, consistent with age, condition and ability to understand • Treatment when present, or refer for treatment • Evaluation of effects of treatments
Relief of Pain • “It is not the responsibility of patients to prove they are in pain; it is the nurse’s responsibility to accept the patient’s report of pain” ( American Pain Society, 2005) • “Relief of pain is a basic human right” (American Pain Foundation,2001) • “Relief of pain is a basic human right” (American Bar Association, 2000)
Ethical Duty of the Nurse • Provide clinically competent, ethically defensible care • Duty to relieve pain, provide humane care • Suspected or known addiction disorder • Give opioids when clinically indicated & ordered • Protect patients/society from unauthorized opioid use • When ethical dilemmas exist, communicate them!
Pain Assessment • Joint Commission Standards PC 01.02.07 Assess, Treat, Reassess, Document Pain • Identifying & treating pain is part of care • Must be assessed during rest and activity • Includes defining: • How patient gets screened • Who assesses pain & when it is reassessed • How pain data is collected & recorded • When in-depth evaluation is needed
Joint Commission • Pain Management Standard • Patients and their families must be educated about pain management plan • Patients need to report pain • Patients need to cooperate with the prescribed treatment • Scope of standard: behavioral health, critical access, home care, hospitals, long-term care and ambulatory care
Patient Barriers • Fear, pessimism, catastrophizing • Pain, effects of drugs, death • Addiction to analgesics • Pain will be intolerable • Anxiety: Cured? • What post-op sensations are normal? • Unrealistic expectations • Interpretation of experience different than team: age, culture, background
Professional Barriers • Mistaken beliefs about pain & treatment • Inconsistent assessment & reassessment • Systems barriers ( computers, access to resources) • Inadequate “handoff” communication • Biases, attitudes
Other Barriers • Self-reports in pre-op are limited • Misunderstandings of pain scales • Over-reporting/underreporting of pain • When to assume pain is present/relieved? • Patients unable to report pain using usual self-report tools ( infants, unconscious, cognitively impaired, ventilated, impending death
Pediatrics Behavioral Tool • Difficult to distinguish pain from fear • Rely on parent reports • Observe behaviors • Can use FLACC: Face, Legs, Activity, Cry, Consolability; 0-2 each with 10 being maximum; Behavioral score only, not intensity rating
NIPS-Neonatal Infant Pain Scale • Facial expression, breathing, arms, legs, cry, state of arousal • CRIES: scale for neonatal 32 weeks to term; Cry, Requires Oxygen, Increased vitals, Expression, Sleeplessness
CPOT • Critical Care Pain Observation Tool • 0-8 behavioral scale • 2 points for each category: • facial expression • body movements • muscle tension • ventilator tension or verbalization
Cognitive Impaired • Assess at rest and activity • Insure functioning hearing aid • Have eyeglasses handy • Repeat questions and allow time for responses • Enlarged font helps • Self-report with descriptors, not numbers! • Consider behaviors: eating, sleeping, mood, body movement
Special Considerations • Elderly: pain prevalence 2-fold higher >60 • Report of pain altered • Have acute & chronic painful diseases • Take many medications • Have multiple diseases • ^ sensitivity: therapeutic, toxic drug effects • Prone to constipation (opioids) • NSAIDs;> risk GI, renal, platelet problems • > Sensitivity to analgesic effects: higher peek effect, longer duration, dose titration
Special Considerations • Known/suspected chemical dependency: • Experience variety of health problems • Possible withdrawal from opioid absence, causing > HR, restlessness, sleeplessness • Focus on managing PAIN , not detoxification! • Don’t forget non-drug interventions • Higher loading & maintenance doses of opioids may be required to reduce pain intensity
ASPMN Position Statement • Pain Assessment in non verbal patients • When possible, obtain self-report • Look for possible pathologies, procedures or other causes of pain • Observe for behaviors that may indicate presence of pain • Obtain input from caretakers who know patient & usual behaviors & responses to pain • Use an analgesic trial & observe for changes in behavior
ASPAN Clinical Guideline • Introduced in JOPAN in 2003, available now on ASPAN web site • Speaks to Assessment, Interventions and Expected Outcomes • Includes all phases of practice including: Preoperative Phase, Post Anesthesia Phase I, and Post Anesthesia Phase II or Extended Observation
Assessment Begins With… • Pre-op Data: • Vital signs & comfort goals • Medical history • Pain history • Pain behaviors • Analgesic history • Patient’s preferences • Pain/comfort acceptable levels • Comfort history • Cultural, religious factors • Educational needs
Interventions Begin in… • Pre-op: • Discuss pain & comfort assessment • Discuss with patient/family about reporting pain & available pain relief • Dispel misconceptions about pain & pain management • Encourage preventive approach • Educate purpose of meds & non-pharmacological measures • Discuss outcomes based on goals • Arrange for interpreter, signer as needed
Outcomes to Strive For! • Pre-op • Patient states understanding of care plan • Patient states understanding of pain intensity scale, pain relief/comfort goals • Patient establishes realistic & achievable pain relief/comfort goals • Patient understands PCA equipment • Patient understands benefit of non-drug interventions
Post anesthesia Phase I • Assessment: • Type of surgery, anesthesia technique, etc • Analgesics, etc given inter-op • Pain & comfort levels • Status/ vital signs: ABCD • Age, cognitive ability & cognitive learning method • ASSESSMENT DATA!
Assessment Data • Subjective data: who, what, where, why & when are first clues of pain assessment • Objective data: observation of facial grimace, teeth clenching, frowning, moaning, crying • Physiological changes: increase BP, rise in HR, increase in RR are signs that support the patient’s subjective pain response
Other Physiological Signs • Dilatation of pupils and/or wide opening of eyelids • Shivering • Change in skin and body temperature • Increased muscle tone • Sweating
ASSESSMENT • Location: examine site • Intensity- use easy, fast, multicultural, multilingual pain scale: • Poker chip, Oucher scale • Visual Analog Scale: pt. places mark on line • Numeric Rating Scale: 0 to 10 • Wong Baker Faces Pain Scale: 3+ to adult • Behavioral Rating Scale • Body Diagram, Daily Diary • Verbal Descriptor Scale: no pain to worse pain
Pain Rating Scales • Purpose: communication tool- here is where you are now and here is where we want you to be • Documenting ratings helps evaluate trends and treatment effectiveness • Know which scale is most appropriate to use ( i.e Wong-Baker preferred by African American children) • Important to have scales translated into languages of populations served