Download
1 / 34
380 likes | 737 Views
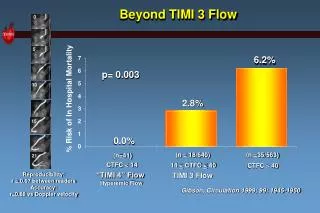
TACTICS-TIMI 18. T reat Angina with A ggrastat + Determine C ost of T herapy with an I nvasive or C onservative S trategy TIMI 18. As presented by Dr. Cannon at AHA 2000. Background and Hypothesis. Unstable angina and non-ST elevation MI: 1.3 million admissions/yr in U.S.A.

E N D
TACTICS-TIMI 18 Treat Angina with Aggrastat + Determine Cost of Therapy with anInvasive or Conservative Strategy TIMI 18 As presented by Dr. Cannon at AHA 2000.
Background and Hypothesis • Unstable angina and non-ST elevation MI: 1.3 million admissions/yr in U.S.A. • Treatment strategies: • Invasive (INV): routine early cath and revasc • Conservative (CONS): stress test if +, cath • Prior trials - mixed results • Current era - improved medical Rx and PCI: use of GP IIb/IIIa inhibitors, stents • 1o Hypothesis: INV strategy will be superior
TIMI IIIB Study Background and Goal • Assess optimal management of unstable angina and non-Q wave MI: Invasive vs. Conservative strategy • Invasive: • Coronary angiography within 18- 48 hours and revascularization as appropriate • Conservative: • Initial medical management and coronary angiography / revascularization only for recurrent ischemia TIMI IIIB Investigators: Circulation 1994;89:1545-56
TIMI IIIBProtocol 1473 Patients with Unstable Angina / NQWMI ASA, IV Heparin, Beta-blockers, Nitrates, Ca++ blockers Randomize Early Conservative: ST segment Holter ETT Thallium Pre-D/C Cath/PTCA if +ischemia Early Invasive: Cath 18-48 h PTCA/CABG prn ETT 6 weeks Primary Endpoint: Death, MI, Positive ETT - 6 weeks Circulation 1994;89:1545-56 Follow-up 1 year
TIMI IIIB Invasive vs. Conservative Early invasive strategy- Cath in all patients between 18-48 hours. Revascularization when feasible based on anatomy: • PTCA for 1 or 2 VD • CABG for 3VD • Early conservative strategy- • Cath if patient had recurrent ischemia at rest or on testing: • Recurrent ischemia at rest with ECG changes • Recurrent MI • Positive ETT or Thallium • Positive ST segment holter TIMI IIIB Investigators: Circulation 1994;89:1545-56
TIMI IIIB Primary Results to 42 days TIMI IIIB Investigators: Circulation 1994;89:1545-56 Cannon, C. et. al. Unpublished data
TIMI IIIB One Year Results Death or MI Early Conservative 12.2% 10.8% Early Invasive P=NS Weeks Anderson HV et al., JACC 1995;26:1643-1650.
TIMI IIIB One Year Results PTCA or CABG Early Invasive 64% 58% Early Conservative % of Patients P=<0.001 Weeks Anderson HV et al., JACC 1995;26:1643-1650.
VANQWISH Trial VA Hospitals Study: Management post Non-Q wave MI Combined Endpoint Death Rates Non-fatal MI Rates Conservative 15 15 25 p=0.05 p=0.025 Invasive 20 10 10 15 Percent p=0.004 p=0.007 10 5 5 5 0 0 0 Discharge 12 mo Discharge 12 mo Discharge 12 mo Boden WE: Presented at the ACC Scientific Sessions 1997, Anaheim CA
Surgical Medical P value n=237 12% 29% 46% 0.44 NS 0.04 Mortality 2 years 8 years Subgroup Refractory angina+Low EF VA Unstable Angina Cooperative Study CABG vs. Medical Therapy for Unstable Angina n=231 10% 28% 13% Luchi et al NEJM 1987;316:977-84; Sharma et al. Circulation 1991;84:III-260-7.
RITA-2 Trial PTCA vs. Medical Management of 1018 Stabilized Angina Patients Presence of 2+ Angina PTCA Medical P value No. Pts Death or MI Death Non-fatal MI 504 6.3% 2.2% 4.2% 514 3.3% 1.4% 1.9% 0.02 0.32 0.04 PTCA Medical 40 30 % 20 10 0 3 mo. 2 yr RITA-2 Trial Participants: Lancet 1997;350:461-8.
TIMI IIIB 1 year VANQWISH 1 year MATE 2 years FRISC II 6 months Prior Trials: Invasive vs. Conservative P=0.025 24.0% P=0.6 18.6% P=0.42 P=0.031 14% 12.2% 12.1% 12% 10.8% 9.4% N=1473 N=920 N=201 N=2457 In-hospital Procedures Cath 98% 57% 96% 48% 100% 58% 96% 10% Revasc 60% 40% 44% 33% 60% 37% 71% 9%
Comparison to Prior Trials TIMI 3 VANQWISH FRISC II TACTICS- TIMI 18 INV Stents No No Yes Yes GP IIb/IIIa No No No Yes Cath Timing 24 hrs 2-4 days 4 days 24 hrs CONS ETT Nuclear Nuc./Echo ECG Nuc/Echo ST criteria 1mm 1mm 3mm 1mm In-hosp Cath 57% 24% 10% 50% Result Early INV INV < Del. INV Early INV =Select. CONS > Very ? Select. INV CONSINV
AHCPR Unstable Angina Guideline Recommendations Cardiac Catheterization / Revascularization: “This guideline proposes two alternative definitive treatment strategies termed “early invasive” and “early conservative”. “Randomized trial data did not support inherent superiority of either strategy based on medical outcomes.(TIMI IIIB) The decision about which strategy to pursue for a given patient should be based on the patient’s estimated risk, available facilities, and patient preference.” AHCPR Guideline 1994
AHCPR Unstable Angina Guideline Recommendations • Cardiac Catheterization / Revascularization: • Early invasive strategy - cath in all patients OR • Early conservative strategy - catheterization if patient had a high-risk indicator: • Persistent or recurrent ischemia • Positive ETT / nuclear imaging scan • CHF or LV dysfunction (EF < 50%) • Prior PTCA or CABG • Malignant ventricular arrhythmias • CABG recommended if: • Left Main > 50% or 3 VD and LV dysfunction Braunwald E. et al. Circulation 1994;90:613-622
Trial Organization TIMI Study Group Christopher Cannon, MD Brigham and Women’s Hosp. Eugene Braunwald, MD Carolyn McCabe, BS Economic Data Coordination William Weintraub, MD Emory University Claudine Jurkovitz, MD, MPH Elizabeth Mahoney, ScD Sponsor - Merck: Laura Demopoulos, MD Peter DiBattiste, MD Debbie Robertson, RD MS Paul DeLucca, Ph.D. Data Center- Quintiles Josh Davis Serum Marker Core Lab Nader Rifai, Ph.D. Angiographic Core Lab C. Michael Gibson, MD
Eligibility Criteria • INCLUSION CRITERIA: • Accelerating pattern, prolonged or recurrent anginal pain at rest or minimal effort <24 hrs • At least 1 of the following: • Ischemic ECG changes • Elevated cardiac markers (local) • History: MI, CAD, PCI, CABG • MAJOR EXCLUSION CRITERIA: • Age < 18 years • Acute STEMI or thrombolytic < 24h • Increased bleeding risk (Hx. Plts, GI bleed) • Killip Class III or IV
TACTICS-TIMI 18 Study Design PCI/ CABG Early Invasive Angio Medical Rx UA/ NSTEMI ASA, Hep,Tirofiban Endpoints Early Conservative Baseline Troponin Medical Rx ETT +ischemia Chest pain Cath/ PCI/ CABG Randomize -24 hrs Hour 0 6 mos 4- 48 108 hrs hrs
Early invasive strategy Cath between 4 and 48 hours Revasc if suitable anatomy Early conservative or “selective invasive” strategy Catheterization if: Refractory angina (>10m rest CP, + ECG ’s) Hemodynamic instability + ETT (ST >1mm, BP, multiple defects, +Echo) New MI or Rehospitalization for UA CCS Class III or IV angina and + ETT Treatment Strategies
1o Endpoint: Death, MI, Rehosp for ACS to 6 mos (100% CEC; MI:CK-MB>ULN, >3xULN p PCI) Power: Invasive strategy will be superior80% power to detect a 25% diff. Sample size: 1720, planned recalculation on blinded data after 50% patients: 2220 patients Troponin hypothesis: added benefit in Tn + Pts Follow-up: 99% complete Analyses: ITT Statistics
Baseline Characteristics INVCONS 62 62 44 43 65 67 77 78 68 66 28 27 39 38 48 47 38 37 56 53 N = 2220 % % Age (years) Age > 65 Male White Prior ASA Diabetes ST ’s ECG ’s NSTEMI TnT >0.01 ng/ml
Protocol Implementation Cath/ Revasc - Initial Hosp (%) CONSINV Cath* 51 97 PCI 24 41 CABG** 13 19 Any Revasc 36 60 Revasc6 mos. 44 61 *Duration tirofiban pre-cath (mean): INV: 24 h **30-day post-CABG mortality = 3.6%
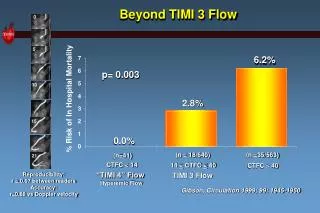
19.4% 15.9% O.R 0.78 95% CI (0.62, 0.97) p=0.025 CONS INV Primary Endpoint Death, MI, Rehosp for ACS at 6 Months 20 16 % Patients 12 8 4 0 0 1 2 3 4 5 6 Time (months)
INV (%) 1114 7.4 4.7 2.2 3.1 3.4 Cardiac Events at 30 Days CONS (%) OR P value No. Pts 1o Endpoint Death/MI Death MI Rehosp ACS 1106 10.5 7.0 1.6 5.8 5.5 0.67 0.65 1.40 0.51 0.61 0.009 0.02 0. 29 0.002 0.018
Cardiac Events at 6 Months CONS (%) INV (%) OR P value No. Pts 1o Endpoint Death/MI Death MI Rehosp ACS 1106 19.4 9.5 3.5 6.9 13.7 1114 15.9 7.3 3.3 4.8 11.0 0.78 0.74 0.93 0.67 0.78 0.025 <0.05 0.74 0.029 0.054
0 0.5 1 1.5 Subgroups: Primary Endpoint Death, MI, Rehosp ACS at 6 Months CONS INV (%) (%) 19.4 15.3 19.6 17.0 17.8 14.9 21.7 17.1 27.7 20.1 16.4 14.2 26.3 16.4 15.3 15.6 19.4 15.9 1O Endpoint %Pts Men (66%) Women (34%) Age < 65 yrs (57%) Age > 65 yrs (43%) Diabetes (28%) No diabetes (72%) ST * (38%) No ST (62%) Total Population *Interaction P=0.006 others P=NS INV Better CONS Better
Troponin T: 1oEP at 6 months Death, MI, Rehosp ACS at 6 Months CONS INV * OR=0.52 *p<0.001 Interaction P<0.001 p=NS (%) N=414 N=396 N=463 N=495 TnT cut point = 0.01 ng/ml (54% of Pts TnT +)
TIMI UA Risk Score: 1oEP at 6 mos OR=0.55 CI (0.33, 0.91) CONS INV OR=0.75 CI (0.57, 1.00) Death/MI/ACS Rehosp (%) TIMI Risk Score % of Pts: 25% 60% 15%
CONS (%) 1106 10.3 49.4 0.5 3.3 (1.3) 6 8.3 Additional Outcomes - 6 Months INV (%) OR P value No. Pts Rec. UA + ECG Rec. UA - ECG Stroke Major bleed (TIMI Major) Init. LOS (median, mean, days) 1114 6.3 32.3 0.5 5.5 (1.9) 5 7.4 0.58 0.49 1.0 1.6 1.5 - 0.001 <0.001 NS 0.01 NS <0.001
Comparison to Prior Trials TIMI 3 VANQWISH FRISC II TACTICS- TIMI 18 INV Stents No No Yes Yes GP IIb/IIIa No No No Yes Cath Timing 24 hrs 2-4 days 4 days 24 hrs CONS ETT Nuclear Nuc./Echo ECG Nuc/Echo ST criteria 1mm 1mm 3mm 1mm In-hosp Cath 57% 24% 10% 50% Result Early INV INV < Del. INV Early INV =Select. CONS > Very ? Select. INV CONSINV
Pts with UA/NSTEMI (+ ECG/+ markers/CAD), “upstream” Rx with GP IIb/IIIa inhibitor tirofiban Early invasive strategy results in significant reduction in major cardiac events (Death/MI/ Rehosp for ACS) “Troponin hypothesis” confirmed: Tn useful in choosing strategy, benefit of INV if Tn + TIMI Risk Score: Intermediate- and high-risk Pts: INV superior Low risk Pts: INVandCONSequal TACTICS-TIMI 18: Conclusions
Possible mechanisms: Benefit of earlyINV - prevents events compared with “wait and see” approach Upstream tirofiban improved INV strategy Results of TACTICS-TIMI 18 suggest need to Update ACC/AHA UA/NSTEMI Guidelines Change clinical management of UA/NSTEMI:broader use of an early invasive strategy with GP IIb/IIIa inhibition EQOL being analyzed: W. Weintraub – ACC 2001 TACTICS-TIMI 18: Conclusions