Download
1 / 30
410 likes | 2.16k Views
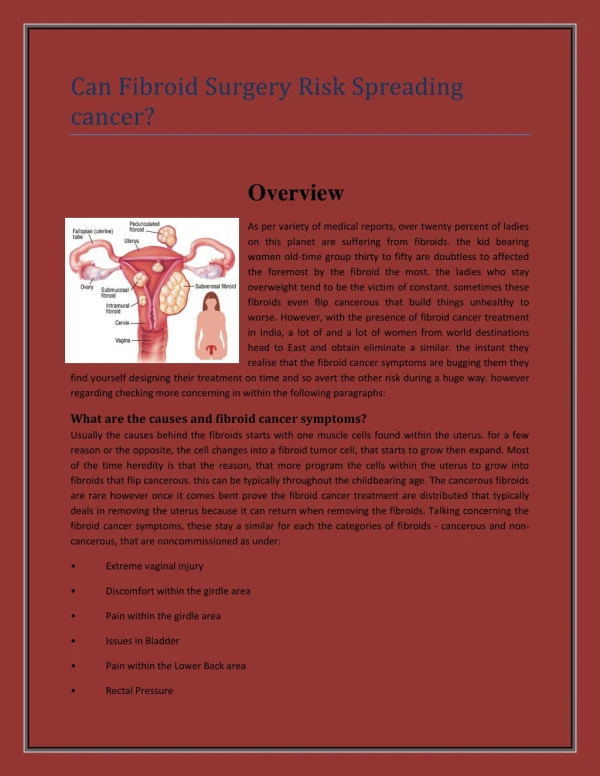
Leiomyoma, Uterus (Fibroid). By:. Ali azizi Alborz hedayati. Leiomyoma, Uterus (Fibroid). Leiomyomas are benign tumors of the uterus. Arise from the overgrowth of smooth muscle and connective tissue in the uterus. A genetic predisposition exists. Female>30(25-50%).

E N D
Leiomyoma, Uterus (Fibroid) By: Ali azizi Alborz hedayati
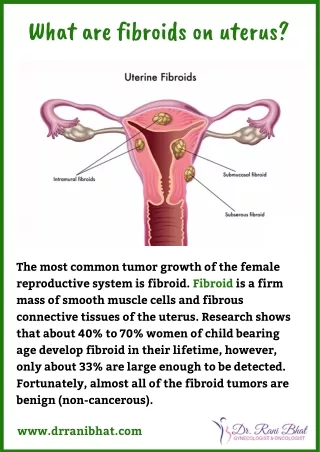
Leiomyoma, Uterus (Fibroid) Leiomyomas are benign tumors of the uterus Arise from the overgrowth of smooth muscle and connective tissue in the uterus A genetic predisposition exists Female>30(25-50%)
Leiomyoma, Uterus (Fibroid) Evidence of an apparent hormonal dependency includes the following: 1-Estrogen and progestin receptors are present in fibroids 2-Elevated estrogen levels may cause fibroid enlargement. During the first trimester of pregnancy, 15-30% of fibroids may enlarge and then shrink in puerperium. Some fibroids may decrease in size during pregnancy 3-Fibroids shrink after menopause .y4-Some regrowth may occur with hormonal therap
Leiomyoma, Uterus (Fibroid) Complications during pregnancy include • Spontaneous abortion • Intrauterine growth retardation • Preterm labor • Uterine dyskinesia • Inertia during labor • Obstruction of the birth canal • Postpartum hemorrhage • Hydronephrosis
Leiomyoma, Uterus (Fibroid) Anatomy Most leiomyomas occur in the fundus and body of the uterus; only 3% occur in the cervix. The fibroids may be solitary, multiple, or diffuse
There are three primary types of uterine fibroids, classified primarily according to location in the uterus: Leiomyoma, Uterus (Fibroid) There are three primary types of uterine fibroids, classified primarily according to location in the uterus:
Leiomyoma, Uterus (Fibroid) Clinical Details Most women with fibroids are asymptomatic. Only 10-20% of patients require treatment Fibroid symptoms are related to the number of tumors, as well as to their sizeandlocation 1 Bleeding: (Menorrhagia)(Most common) 2 Pain 3 Pressure
Leiomyoma, Uterus (Fibroid) Bleeding: (Menorrhagia)(Most common) Menorrhagia may result in severe anemia and can be life threatening, although this is rare. Menorrhagia usually results from the erosion of a submucosal fibroid into the endometrial cavity. Rarely, dilated veins on the surface of a subserosal, pedunculated fibroid can cause sudden, massive intraperitoneal bleeding
Leiomyoma, Uterus (Fibroid) Pain Women may experience abdominal cramping. Pain usually is felt during menstruation. Less often, pain occurs intermenstrually Pressure Urinary frequency, urgency, and/or incontinence result from pressure on the bladder Constipation, difficult defecation, or rectal pain results from pressure on the colon
Leiomyoma, Uterus (Fibroid) Differential diagnosis Normal ovary - May be confused with fibroids at US Ovarian mass - Hemorrhagic cyst, endometrioma, dermoid, cystadenoma, malignant tumorUterine leiomyosarcoma - Rare, arise de novo or as a result of the malignant degeneration of a uterine fibroidAdenomyosis - May be difficult to distinguish from multiple small fibroidsMyometrial contraction - Especially during pregnancyNecrotic fibroids - May mimic intrauterine gestational sac, intrauterine fluid collection, hydatiform mole
Leiomyoma, Uterus (Fibroid) Radiogrph findings: Conventional radiographs have a limited role in the diagnosis of uterine fibroids Unless heavily calcified, fibroids are not depicted on radiographs CT findings CT scanning has a limited role in the diagnosis of uterine fibroids On CT scans, fibroids are usually indistinguishable from healthy myometrium unless they are calcified or necrotic Calcifications may be more visible on CT scans than on conventional radiographs because of the superior contrast differentiation with CT scanning
Leiomyoma, Uterus (Fibroid) Sonography US is the imaging modality of choice in the detection and evaluation of uterine fibroids The most frequent US appearance is that of a concentric, solid, hypoechoic mass These solid masses absorb sound waves and therefore cause a variable amount of acoustic shadowing
Leiomyoma, Uterus (Fibroid) Sonogram shows the subserosal, 2.3- to 2.5-cm, right anterior fundal uterine fibroid
Leiomyoma, Uterus (Fibroid) They can be heterogeneous or hyperechoic, depending on the amount of fibrous tissue and/or calcification Sagittal sonogram shows a posterior, fundal, 4.2 X 3.5-cm intramural uterine fibroid
Leiomyoma, Uterus (Fibroid) CT scan shows a subserosal, 2.3- to 2.5-cm, right anterior fundal uterine fibroid
Leiomyoma, Uterus (Fibroid) MRI findings: MRI has an important role in defining the anatomy of the uterus and ovaries Fibroids are sharply marginated areas of low-to-intermediate signal intensity on T1- and T2-weighted MRI scans
Leiomyoma, Uterus (Fibroid) One third of fibroids have a hyperintense rim on T2-weighted images as a result of dilated veins, lymphatics, or edema. Sagittal T2-weighted MRI shows that the largest fibroid is located in the lower uterus and has a partially hyperintense rim. A smaller discrete fibroid is depicted in the fundus
Leiomyoma, Uterus (Fibroid) Axial MRI shows the cross section of the larger fibroid in the lower uterus. Note the mass effect on the bladder, which is located anteriorly
Leiomyoma, Uterus (Fibroid) An inhomogeneous area of high signal intensity may be depicted on T2-weighted images; this results fromhemorrhage, hyaline degeneration, edema, or highly cellular fibroids
Leiomyoma, Uterus (Fibroid) The intravenous administration of gadolinium-based contrast material usually is not required if it is administered, fibroids usually enhance later than does the healthy myometrium. Fibroid enhancement can be hypointense (65%), isointense (23%), or hyperintense (12%) in relation to that of the myometrium MRI has a sensitivity of 86-92%, a specificity of 100%, and an accuracy of 97% in the evaluation of probable fibroids