Download
1 / 22
360 likes | 2.96k Views
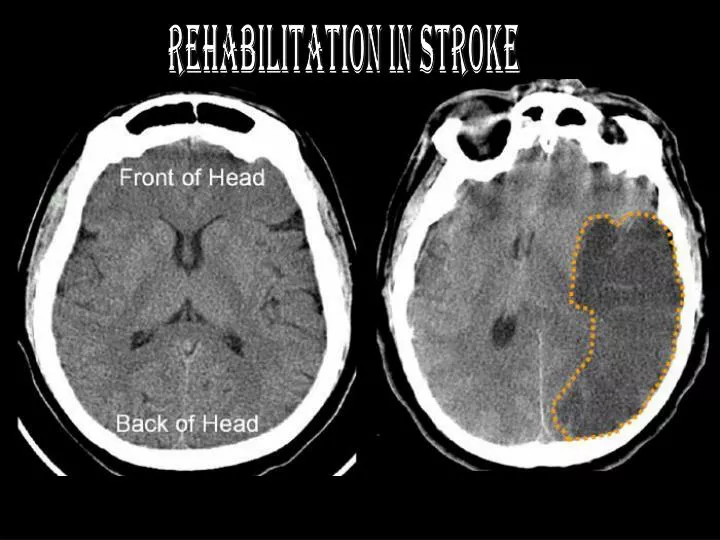
Rehabilitation in Stroke. Norma Wright. ~ A CASE STUDY ~. The Feedback System. Differential diagnosis and degree of involvement will vary from patient to patient…. What work’s for YOUR patient?. One Step At A Time…. Stage 1 : Flaccidity

E N D
Norma Wright ~ A CASE STUDY ~
The Feedback System • Differential diagnosis and degree of involvement will vary from patient to patient… What work’s for YOUR patient?
One Step At A Time… • Stage 1: Flaccidity No voluntary or reflexive activity is present in either involved limb. Associated reactions cannot be elicited. • Stage 2: The basic movement synergies or some of their components may be elicited reflexively as associated reactions. Minimal voluntary motion present. Spasticity, first seen as resistance to passive stretch, begins to develop
Stage 3: Spasticity becomes more marked. The basic movement synergies may be performed voluntarily, although full range of all components may be lacking. • Stage 4: Movements which deviate from the basic synergies can be accomplished on a volitional basis. Spasticity begins to decline.
Stage 5: Basic synergies lose their dominance over volitional behavior and the patient becomes increasingly more adept at performing movement combinations which differ greatly from the synergies. Spasticity continues to decrease. • Stage 6: Spasticity is essentially absent. Isolated muscle actions can be performed freely. • Stage 7: Restoration of normal motor function
And Then Comes the But… • Recovery may be arrested at any stage depending on severity of insult, degree of sensory involvement, etc. • A stage in the recovery process is never skipped. However, in cases of slight damage, recovery may proceed so rapidly that certain stages may not be observable • Associated reactions, particularly the basic movement synergies, may still appear under stress conditions such as sudden fright, anxiety, sneezing, loud noises, etc.
Treatment Approach
Different Approaches • Muscle Re-education Approach (1920s) • Neurodevelopmental Approaches (1940-70s) • Sensorimotor Approach (Rood, 1940s) • Movement Theory Approach (Brunnstrom, 1950s) • NDT Approach (Bobath, 1960-70s) • Motor Relearning Program for Stroke (1980s) • Contemporary Task-Oriented Approach (1990s)
“But TONY !?Which one do I use?” "The Ecletic Approach"
Muscle Re-education Approach • Ultimate Goal = Development of coordinated movement patterns. Training begins with learning the control of individual muscles on a cognitive level
Rood’s Sensorimotor Approach • Involves superficial cutaneous stimulation using stroking, brushing, icing, or muscle stimulation with vibration, tendon tapping, and joint compression to evoke voluntary contraction or inhibition of proximal muscles
Brunnstrom’s Approach • Emphasised the synergistic patterns of movement that develop during recovery from hemiplegia. She encouraged flexor and extensor synergies during early recovery, hoping that synergistic activation of muscle would, with training, transition into voluntary activation. • Patients are taught to use and voluntarily control the motor patterns available to them at a particular point during their recovery process • Enhances specific synergies through use of cutaneous/proprioceptive stimuli, and central facilitation.
Synergies UE
Synergies LE
Raimiste’s Phenomenon • Homolateral Limb Synkinesis • Tonic Neck Reflexes • Tonic Labryinthine Reflex • Tonic Lumbar Reflex Combine Reflexes!
Associated Reactions • UE: • Flex of uninvolved = Flex of involved • Ext of uninvolved = Ext of involved • LE: • Flex of uninvolved = Ext of involved • Ext of uninvolved = Flx of involved • INVOLVED: • Flex = Flex • Ext = Ext
Bobath’s NeurodevelopmentalTechnique Approach(NDT) • GOAL • Normalize tone by inhibiting spasticity • Inhibit primitive patterns of movement • Facilitate autonomic, voluntary reactions and subsequent normal movement patterns *Suppress abnormal muscle patterns before normal patterns are introduced…* Mass synergies avoided because although they may strengthen weak, unresponsive muscles, they reinforce abnormally increased tonic reflexes (spasticity)
RIP – Reflex Inhibiting Posture • In Sitting… • Symmetry with head in midline • Trunk in midline • Pelvis in neutral position • Hips in line with knees (90 degrees – break ext tone) • Balls of feet under knees • UE relaxes with elbows at 90 deg of flex but not fully ext, hands on knees, palms down towards supination with fingers open
Knott and Voss’ PNF ApproachProprioceptive Neuromuscular Stimulation • Uses spiral and diagonal components of movement rather than traditional movements in cardinal planes of motion • GOAL • Facilitating movement patterns that will have more functional relevance than the traditional technique of strengthening individual group muscles • Relies on quick stretching and manual resistance of muscle activation of the limbs in functional directions.
Sitting & Standing Balance • Static Balance • Rhythmic Stabilization • Dynamic Stabilization • Available ROM for Standing