Download

1 / 14
150 likes | 412 Views
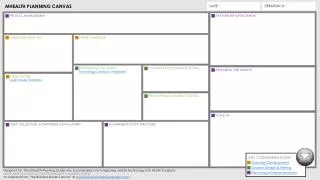
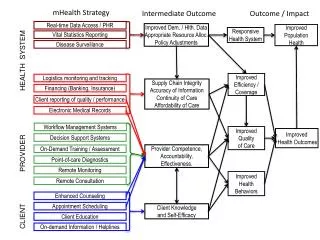
mHealth. mHealth. Patient Centered. Aggregate. Program tracking. Clinical Use. Routine reporting. Medical Sensors. Low-end Phone. SMS-reminders. Diagnostic tool. Treatment Support. Smartphone. Voice consultation. Use case Types of mobile application & data bearer.

E N D
mHealth Patient Centered Aggregate Program tracking Clinical Use Routine reporting Medical Sensors Low-end Phone SMS-reminders Diagnostic tool Treatment Support Smartphone Voice consultation
Use case Types of mobile application & data bearer • Plaintext SMS • Structured SMS • SIM-apps • “GPRS-apps” (Java J2ME) • Mobile Browser – offline/online • Voice! • Interactive voice response (IVR) Paper is still a viable option in many contexts!
Sheet to help compose SMS message: TEST. 8. 0. 0. 8. 7. 3. 4
Aggregate data: routine reporting of health data from facilities/communities Robust Available Not so prone to theft sometimes privately owned Long standby time on one charge (e.g. with small solar panel) Local service /maintenance competence Local mobile phone literacy Mobile coverage [ where there is no road, no power, no fixed line phone] Low End Mobile Phones
mHealth & HMIS goals Timeliness Assist local decision making based on accurate data on time NB: Not all solutions have to be measurable in terms of improved health service quality. Cost effective HMIS is also important
How can mobiles improve HMIS? Data Quality - Validation rules on phone On the spot data capture and transfer Save time and reduce mistakes caused by manual collation and transfer of data mHealth application areas • Routine data (HMIS) • Notifiable Diseases (IDSR) • Individual “Tracking” => aggregate • Stock-outs • Individual health monitoring • Reminders • Etc.
Types of mHealth data Name based/program tracking (ANC, HIV, TB) or aggregate data (ISDR & routine HMIS) CHALLENGES • Security of identifiable patient data • Complexity of work routine (not easy to capture on a small screen – or any screen) • mHealth - Additional burden or Helpful tool?
mHealth; empowering health workers or job surveillance? Integrate with GIS/GPS – for disease surveillance or can be used for task force surveillance and control [Example: daily reporting Punjab] Some managers would love to have a camera-drone following their health workers 24-7!
Missing Feedback in HMIS Supervision feedback only when there are errors, mistakes, shortcomings Supervision is often irregular and non-supportive and requires time & resources Mobile “Feedback” (access to processed data) • Progress over time • Comparisons to other organization units [vertical/horizontal] • HMIS metadata – completness, timeliness % • Push or Pull?
What’s in it for the end users? Save money and time spent on travel [maybe!] More time for service provision [ideally…] Closed User Group (CUG) agreement with mobile operator = free communication with colleagues! Processed data ”Feedback” Phone Credit top-up/ reimbursements/bonus
Problems with mHealth Pilots Additional burden for health workers Donor short attention span - unsustainable What works as a pilot does not necessarily scale Pilots may focus on technical feasibility while ignoring larger organizational and political mechanisms (e.g. health worker unions) Hard to evaluate and-compare across mHelath projects
Partners in mHealth “Ecosystem of actors”: Ministry of Health, NGOs, researchers, Programme Donors &… Mobile Operators • Network coverage • Closed User Group Agreement • Social responsibility or New revenue streams? BUT mHealth Initiative may get stuck with one operator! Win-Win-Win?