Download
1 / 1
190 likes | 639 Views
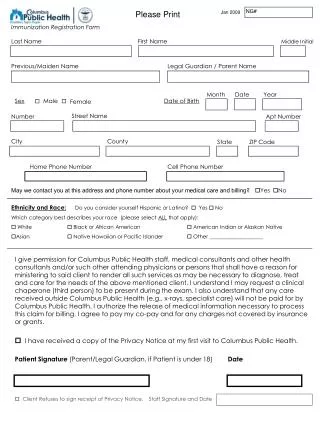
REGISTRATION FORM. Name : ________________________________________ Nickname : ____________ Last name First name M.I. Age : ___ Birthday : _ _/ _ _/_ _ _ _ Sex : ___ Civil Status : ___ Nationality : _________

E N D
REGISTRATION FORM Name : ________________________________________ Nickname : ____________ Last name First name M.I. Age : ___ Birthday : _ _/ _ _/_ _ _ _ Sex : ___ Civil Status : ___ Nationality : _________ Home Address : _____________________________________________________________ Home Phone No. : _______________________ Mobile No. : ________________________ Occupation : _______________________ Business/school: ________________________ Business//school address : _____________________________________________________ Business Phone no. : _________________________ Fax No. : ______________________ Email Address : ___________________________ Club Affiliation : ______________________________ Position : ______________________ In case of emergency: Contact person : ______________________________ Relation : _____________________ Address : __________________________________________ Phone No. : _____________ WAIVER I, __________________________________, of legal age and a resident of _____________________________________________________, hereby hold Philippine Airlines Mountaineering Club (PALMC) and/or any of their authorized representative or agents free and harmless from and against any and all lawsuits, losses, damages or liabilities of whatever kind and nature arising from my participation in the 25th MFPI Congress. I understood and accepted the fact that the activities in the 25TH MFPI CONGRESS have inherent danger and risks; that I was properly oriented on the terms and conditions on my participation on the said event and I am taking full responsibility and willingly accept without prejudice to the PALMC and/or any of their authorized representative all the risks and dangers involved out of my said participation. This is also to certify that all information I have given here are true and correct. __________________________________ __________________________ Affiant signature over printed name Date _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ (SECRETARIAT USE) Date paid : _________________ O.R. No. : _______________ Mode : _____________ _______________________________ Authorized Representative Signature