Download
1 / 1
10 likes | 166 Views
No. 173. Active surveillance for prostate c ancer : Early experience in a regional c entre. Rahil Nagpal , Daniel Gilbourd , Mark Louie- Johnsun Department of Urology, Gosford , Wyong and Gosford Private Hospitals. Posters Proudly Supported by:. Introduction

E N D
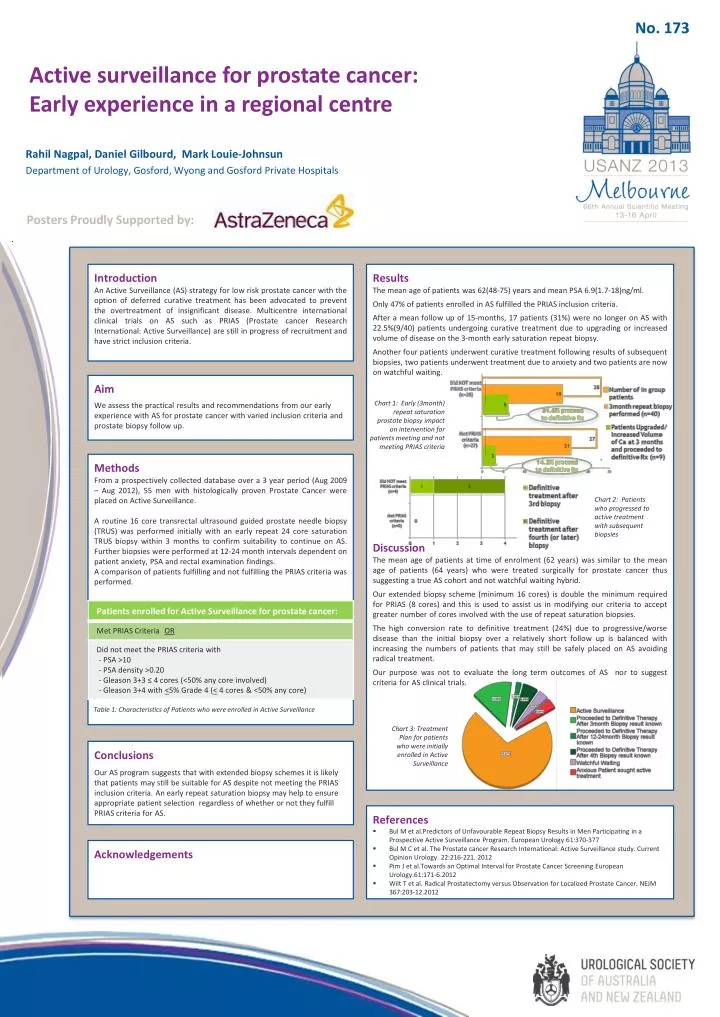
No. 173 Active surveillance for prostate cancer: Early experience in a regional centre RahilNagpal, Daniel Gilbourd, Mark Louie-Johnsun Department of Urology, Gosford, Wyong and Gosford Private Hospitals Posters Proudly Supported by: Introduction An Active Surveillance (AS) strategy for low risk prostate cancer with the option of deferred curative treatment has been advocated to prevent the overtreatment of insignificant disease. Multicentre international clinical trials on AS such as PRIAS (Prostate cancer Research International: Active Surveillance) are still in progress of recruitment and have strict inclusion criteria. Results The mean age of patients was 62(48-75) years and mean PSA 6.9(1.7-18)ng/ml. Only 47% of patients enrolled in AS fulfilled the PRIAS inclusion criteria. After a mean follow up of 15-months, 17 patients (31%) were no longer on AS with 22.5%(9/40) patients undergoing curative treatment due to upgrading or increased volume of disease on the 3-month early saturation repeat biopsy. Another four patients underwent curative treatment following results of subsequent biopsies, two patients underwent treatment due to anxiety and two patients are now on watchful waiting. Discussion The mean age of patients at time of enrolment (62 years) was similar to the mean age of patients (64 years) who were treated surgically for prostate cancer thus suggesting a true AS cohort and not watchful waiting hybrid. Our extended biopsy scheme (minimum 16 cores) is double the minimum required for PRIAS (8 cores) and this is used to assist us in modifying our criteria to accept greater number of cores involved with the use of repeat saturation biopsies. The high conversion rate to definitive treatment (24%) due to progressive/worse disease than the initial biopsy over a relatively short follow up is balanced with increasing the numbers of patients that may still be safely placed on AS avoiding radical treatment. Our purpose was not to evaluate the long term outcomes of AS nor to suggest criteria for AS clinical trials. Aim We assess the practical results and recommendations from our early experience with AS for prostate cancer with varied inclusion criteria and prostate biopsy follow up. Chart 1: Early (3month) repeat saturation prostate biopsy impact on intervention for patients meeting and not meeting PRIAS criteria Methods From a prospectively collected database over a 3 year period (Aug 2009 – Aug 2012), 55 men with histologically proven Prostate Cancer were placed on Active Surveillance. A routine 16 core transrectal ultrasound guided prostate needle biopsy (TRUS) was performed initially with an early repeat 24 core saturation TRUS biopsy within 3 months to confirm suitability to continue on AS. Further biopsies were performed at 12-24 month intervals dependent on patient anxiety, PSA and rectal examination findings. A comparison of patients fulfilling and not fulfilling the PRIAS criteria was performed. Chart 2: Patients who progressed to active treatment with subsequent biopsies Table 1: Characteristics of Patients who were enrolled in Active Surveillance Chart 3: Treatment Plan for patients who were initially enrolled in Active Surveillance • Conclusions • Our AS program suggests that with extended biopsy schemes it is likely that patients may still be suitable for AS despite not meeting the PRIAS inclusion criteria. An early repeat saturation biopsy may help to ensure appropriate patient selection regardless of whether or not they fulfill PRIAS criteria for AS. • References • Bul M et al.Predictors of Unfavourable Repeat Biopsy Results in Men Participating in a Prospective Active Surveillance Program. European Urology 61:370-377 • BulM C et al. The Prostate cancer Research International: Active Surveillance study. Current Opinion Urology. 22:216-221. 2012 • PimJ et al.Towards an Optimal Interval for Prostate Cancer Screening.EuropeanUrology.61:171-6.2012 • Wilt T et al. Radical Prostatectomy versus Observation for Localized Prostate Cancer. NEJM 367:203-12.2012 Acknowledgements





![EVM System Surveillance Presented By: [NAMES] Presented to: [GROUP]](https://cdn2.slideserve.com/3705648/slide1-dt.jpg)