Download
1 / 51
510 likes | 761 Views
dementia A brief overview of diagnosis and treatment Amy Sanders MD Assistant Professor of Neurology Einstein Aging Study Einstein-Montefiore Brain Aging Center Albert Einstein College of Medicine. Coming Up. Dementia: definitions Dementia: evaluation Dementia: subtypes

E N D
dementia A brief overview of diagnosis and treatment Amy Sanders MD Assistant Professor of Neurology Einstein Aging Study Einstein-Montefiore Brain Aging Center Albert Einstein College of Medicine
Coming Up • Dementia: definitions • Dementia: evaluation • Dementia: subtypes • Alzheimer’s Disease: diagnosis and Rx • Other Dementia Subtypes: diagnosis and Rx
Hebert LE, Arch Neurol 2003 13.2 million 7.7 million 4.5 million 2050 2000 2030
A species of insanity characterized by failure or loss of the mental powers…….
A syndrome defined by a non-acute decline in cognition that interferes with functioning in everyday living
Multiple cognitive deficits, including MEMORY IMPAIRMENT and at least one of - aphasia (language impairment) - apraxia (impaired motor activity) - agnosia (impaired recognition) - executive function disturbance (planning) Disturbance interferes significantly with work or usual social activities/relationships [“ADLs”]
WHAT ISDEMENTIA? Problem solving Judgment Social skills Memory loss Language MORE THAN 6 MONTHS NO NO
Diagnostic Procedures ? LABS ?IMAGING ?LP ?EEG ?GENETIC TESTING
Laboratory Tests • AAN Guideline: B12, thyroid function • AAN Guideline: maybe syphilis serology • AAN Guideline: depression screening • Other labs: CBC, basic chemistry, LFTs, parathyroid
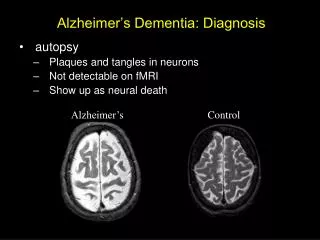
Imaging • Structural Neuroimaging: CT, MRI • Volumetrics: labor-intensive, research • PET: adjunctive, AD vs FTD • Amyoid imaging: PIB, research
Pittsburgh compound B Klunk, et al. Ann Neurol 2004
GENETICS • Not currently recommended for routine clinical diagnosis • Complex genetics for late-onset AD • APOE ε4 allele: susceptibility gene for AD • Progranulin mutations: FTD
Medication Review • MANY medications may worsen cognition • Some anti-hypertensives (ß-blockers, CCBs) • Anti-cholinergics • Prednisone • Digitalis • Opiates/narcotic analgesics • Benzodiazepines • Even NSAIDS
ALZEIMER’S DISEASE • Age-related neurodegenerative disease associated with cognitive decline • Memory, judgment, language • Behavior and mood • Pathology: deposition of amyloid (plaques) and hyperphosphorylation of tau (NF tangles) • Neuronal cell death and impaired neuronal function • ? Complex Genetics, vascular risk factors, Oxidative Stress, inflammation, hormones?
Struldbrugg – race of immortals who “turn to dotage and entirely lose their memories…”
Impaired memory, aphasia, erratic behaviour, paranoia and auditory hallucinations Alzheimer A. Uber eine eigenartige Erkrankung der Hirnrinde. Allgemeine Zeitschrift fuer Psychiatrie 1907; 64:146–8. K. Maurer, S. Volk, H. Gerbaldo.Auguste D and Alzheimer's disease.Lancet 1997; 349: 1546-1549
Why is AD Important? • Incidence rising—longer lifespans • Most common neurodegenerative disease • Most common illness leading to nursing home placement • $156 billion worldwide cost in 2003 • Treatment available • Long-term planning (HCP, long-term care)
Alzheimer’s Disease • NINCDS-ADRDA criteria (probable AD) • Dementia -established by clinical exam, documented by screening tests confirmed by neuropsych tests • Deficits in 2 or more areas of cognition • Progressive worsening of memory/cognition • No disturbance of consciousness • onset 40-90 years, usually > 65y • Absence of other systemic/brain disorders
Ten Warning Signs – Alzheimer Association • Memory loss that affects job skills. • Difficulty performing familiar tasks. • Misplacing things. • Problems with language. • Disorientation to time and place. • Poor or decreased judgment. • Problems with abstract thinking. • Changes in mood or behavior. • Changes in personality. • Loss of initiative. Memory Non-memory
Abnormal behaviors & AD SymptomMonths after memory Calculation defect 25 Language 31 Irritability 39 Gait disorder 47 Wandering 50 Sleep disorder 51 Violence 64 Incontinence 67 Folstein & Bylsma,1999
AD: presentation • Helpful to have informant • Insidious onset of short-term memory complaint • Trouble with names, word-finding difficulty • Getting lost, forgetting parking location • Trouble calculating – e.g. tips, checkbook • Planning – recipes, trip planning
AD: behavioral components • Apathy – loss of initiative • Depressive symptoms – up to 30% • Anxiety • Paranoia, delusions – later stage disease • Agitation – late disease
AD: Treatment • Treat the disease: pharm and nonpharm • Treat the collateral sx – behavior, mood • Take care of the caregiver -respite -health lit
AD Pharmacotherapy • Cholinesterase inhibitors -donepezil (Aricept) -galantamine (Razadyne [reminyl]) -rivastigmine (Exelon) • NMDA receptor antagonist • Memantine (Namenda) • Moderate to severe AD, may be additive
Pointers • Discussion with patient/family: expectations • Start low and titrate: for all AChI • Most common side effects: GI (N/V/D) • Can switch agents • Withdraw when no longer benefitting or no longer able to interact with family members
Donepezil • 5 mg qd starting dose (minimum therapeutic dose) • With or without food, take in a.m. • Increase to 10 mg after 4-6 weeks • Half life 70 hours, hepatic metabolism
Galantamine • Start at 8 mg qd (minimum therapeutic = 16 mg) • Take with food (full meal) • Increase to 16 mg after 4 weeks • 24 mg is maximum dose • Most common side effect: GI • If treatment interrupted for more than 1 week, re-start at 8 mg and repeat titration • Half-life 7 hours, hepatic metabolism
Rivastigmine • Start at 1.5 mg BID (minimum therapeutic = 6 mg) • Take with food (full meal) for both doses • Stepwise increase monthly (1.5, 3, 4.5, 6 mg) • 12 mg (6 mg BID) is maximum dose • Most common side effect: GI • If treatment interrupted for more than 1 week, re-start at 1.5 mg BIDand repeat titration • Half-life 90 minutes, renal clearance
Memantine • Start at 5 mg qd • Take with or without food • Stepwise increase weekly by 5 mg • 20 mg (10 mg BID) is maximum dose • Side effects fewer than with AChI (dizzy, HA) • Half-life 70 hours, partial hepatic clearance
Pharmacologic Treatment of Behavioral Symptoms • NOT FIRST LINE • Complicated; generally off-label • Rule out other causes • Start low, go slow. Briefest use possible. • Agitation: atypical neuroleptics, anticonvulsants, benzodiazepines • Depression: SSRIs, S-NE RI, other • Insomnia: trazodone, alprazolam, zolpidem, ramelteon (may cause carryover sedation)
Vascular Dementia • 2nd-most common subtype • May be present even in cases without prominent memory loss • Executive function often predominates • Vascular risk factors • Gait dysfunction
Diffuse Lacunes Multi-infarct
Variations on the Theme • “stroke” dementia • Subcortical pattern: lacunes, severe WMD • CADISIL • Often “mixed” with AD
VaD Treatment • No targeted pharmacologic therapy • Modification of vascular risk factors • Aspirin used anecdotally • Symptomatic treatment of affective symptoms
Central Feature:dementia is ESSENTIAL Core Features: Parkinsonism (spontaneous) Visual hallucinations-recurrent, vivid/detailed Fluctuations-attention and alertness especially Suggestive Features: Severe neuroleptic sensitivity -- worsening REM sleep disorder -- acting out dreams Low dopamine transporter uptake in BG (SPECT/PET) McKeith, Neurology, 2005
DLB Treatment • COMPLICATED • Parkinsonism • Cognition and fluctuations • Hallucinations, psychosis, agitation • REM sleep behavior disorder
“The cold within him froze his old features ... and stiffened his gait.” “…vivid and detailed hallucinations featuring friends and relatives are common. And like Scrooge’s visions, these phantasms are distressing, often terrifying. Finally, in Lewy body dementia, hallucinations occur early in the disease, frequently before the cognitive deficits are apparent.” Sanders, “Diagnosing with Dickens,” Sunday NYT Magazine 12/17/06
Frontotemporal dementias Core • insidious onset, gradual progression • Early decline in social skills • Early decline in regulation of personal conduct • Early emotional blunting • Early loss of insight Supportive Behavioral disorder Speech and language disturbances Physical signs – frontal signs, parkinsonism, labile BP Investigations: neuropsychology, EEG, MRI Neary, Neurology, 1998
Initial-Carving Doctor Banned 'Dr. Zorro' Blamed Brain Disorder for Scarring Patient
FTD Treatment • Few options • AChI not effective, may cause agitation • Perhaps some role for SSRIs • Safety assessment • Depression common in caregivers and can be a reason for earlier nursing home placement