Download
1 / 16
160 likes | 288 Views
Tumour Immunology. Immune surveillance : The immune system surveys the body for malignancies, eliminating tumours or slowing their growth. Cell mediated NK cells MQ :Ag presentation & cytokines (TNF) Tcytotoxic :major effector mechanism γ - δ &mucosacells:skin

E N D
Tumour Immunology Immune surveillance: The immune system surveys the body for malignancies, eliminating tumours or slowing their growth
Cell mediated NK cells MQ:Ag presentation & cytokines (TNF) Tcytotoxic:major effector mechanism γ-δ &mucosacells:skin TH-1: - secrete cytokines maturatingTc cells. - secrete IFN-γ Humoral Complement mediated lysis Ab & compl. mediated opsonization ADCC Loss of adhesive property of tumour cells Mechanisms of tumour destruction
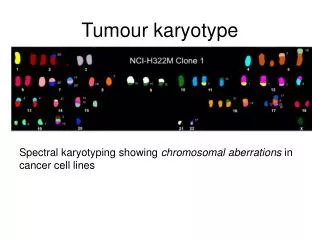
Tumour antigens I- Tumour associated Ags: • Normal cell proteins that are over-expressed in tumour cells or expressed only during fetal life e.g. - Alpha fetoprotein: present in serum of liver cancer patient - Carinoembryonic Ag: present in serum of cancer colon patients
II- Mutant cellular gene products (Tumour specific Ags): • May be products of mutated oncogenes& tumour suppressor genes • May be encoded by oncogenic viruses.Products of those viruses function as tumour Ags, recognized as foreign and can elicit an immune response
Tumour evasion of immune response (escape mechanisms) I- Host related factors 1- Immune status 2- Age extremes • Immunocompromised patients (e.g. AIDS) • Patients on immunosuppressive • therapy (transplantation)
II- Tumour related factors 1- tumour Ag • Defective expression • Masked by fibrin • nonCytotoxic Abs may induce • Ag endocytosis or masking • Maybe free in circulation 2- tumour cells • Lack of costim molecules • Ligands (B7) • Resist FAS/FasL pathway • Release of immunosupp. • Cytokines • Stim. Of suppressor cells • Express FasL to kill TILs 3- immunosuppression
Tumour Immunotherapy • 1- Non specific stim. of IR by thymic hormones &cytokines • 2- Active immunization by purified tumour Ag after reduction of tumour mass by surgery
Adoptive cellular immunotherapy • 3- Passive immunotherapy: • Non specific: lymphokine activated killer cells (LAK) infusion (NK, &CTLs) stimulated in vitro by IL2 • Specific: Bifunctional MABs or preparation of LAK from TILs • Therapeutic MABs either alone or as magic bullets Antibodies
4- genetic manipulation of tumour cells e.g. introduction of IL-2,Tnf, or IFN gene or genes for co-stimulatory molecules B7
Immunological Changes in AIDS Targets: T-helpers& monocyte macrophage cells
I- Decrease CD-4 Tcells number • The progressive loss of CD-4 cells underlies the immune deficiency characterizing HIV infection • The decrease in no. is of diagnostic & prognostic values • Normal: 1000-1500 cell/µL • > 100 cell/µL in advanced disease
Mechanisms of CD-4 cell depletion: • 1- virus mediated killing • 2- immune mediated killing • 3- Auto Abs • 4- impaired CD-4 cell production • 5- other infections e.g. EBV may help as a cofactor in disease progressionby inducing cellular activation & increased virus production
The immune system is unable to replace cell loss • This occurs faster in the absence of antiretroviral therapy Bone marrow Damage of the sites of Tcell production & maturation
II- Decrease CD-4 Tcells function CD4 Tcell • Decreased response to Ag • Decreased cytokine production Bcell Produce exceessive & inappropriate Abs NK Poor performance
III- Anatomic disruption of the immunologic environment • Site for establishment & spread of the virus • Collapse of its architecture • Unable to trap the virus or any other infectious pathogens • HIV spills into the circulation with increased viral load Lymph Node