Download
1 / 1

E N D
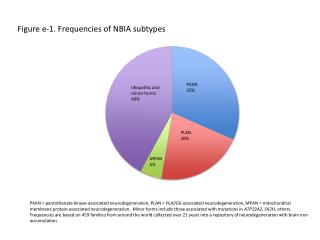
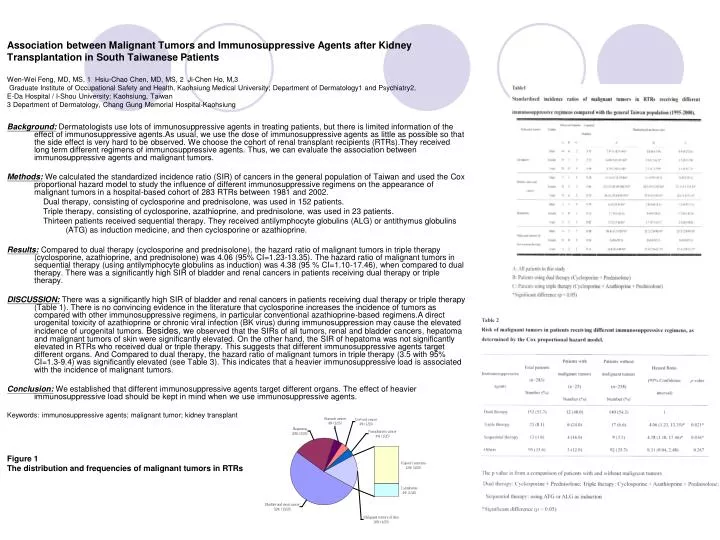
Background: Dermatologists use lots of immunosuppressive agents in treating patients, but there is limited information of the effect of immunosuppressive agents.As usual, we use the dose of immunosuppressive agents as little as possible so that the side effect is very hard to be observed. We choose the cohort of renal transplant recipients (RTRs).They received long term different regimens of immunosuppressive agents. Thus, we can evaluate the association between immunosuppressive agents and malignant tumors. Methods: We calculated the standardized incidence ratio (SIR) of cancers in the general population of Taiwan and used the Cox proportional hazard model to study the influence of different immunosuppressive regimens on the appearance of malignant tumors in a hospital-based cohort of 283 RTRs between 1981 and 2002. Dual therapy, consisting of cyclosporine and prednisolone, was used in 152 patients. Triple therapy, consisting of cyclosporine, azathioprine, and prednisolone, was used in 23 patients. Thirteen patients received sequential therapy. They received antilymphocyte globulins (ALG) or antithymus globulins (ATG) as induction medicine, and then cyclosporine or azathioprine. Results: Compared to dual therapy (cyclosporine and prednisolone), the hazard ratio of malignant tumors in triple therapy (cyclosporine, azathioprine, and prednisolone) was 4.06 (95% CI=1.23-13.35). The hazard ratio of malignant tumors in sequential therapy (using antilymphocyte globulins as induction) was 4.38 (95 % CI=1.10-17.46), when compared to dual therapy. There was a significantly high SIR of bladder and renal cancers in patients receiving dual therapy or triple therapy. DISCUSSION: There was a significantly high SIR of bladder and renal cancers in patients receiving dual therapy or triple therapy (Table 1). There is no convincing evidence in the literature that cyclosporine increases the incidence of tumors as compared with other immunosuppressive regimens, in particular conventional azathioprine-based regimens.A direct urogenital toxicity of azathioprine or chronic viral infection (BK virus) during immunosuppression may cause the elevated incidence of urogenital tumors. Besides, we observed that the SIRs of all tumors, renal and bladder cancers, hepatoma and malignant tumors of skin were significantly elevated. On the other hand, the SIR of hepatoma was not significantly elevated in RTRs who received dual or triple therapy. This suggests that different immunosuppressive agents target different organs. And Compared to dual therapy, the hazard ratio of malignant tumors in triple therapy (3.5 with 95% CI=1.3-9.4) was significantly elevated (see Table 3). This indicates that a heavier immunosuppressive load is associated with the incidence of malignant tumors. Conclusion: We established that different immunosuppressive agents target different organs. The effect of heavier immunosuppressive load should be kept in mind when we use immunosuppressive agents. Keywords: immunosuppressive agents; malignant tumor; kidney transplant Association between Malignant Tumors and Immunosuppressive Agents after Kidney Transplantation in South Taiwanese Patients Wen-Wei Feng, MD, MS, 1 Hsiu-Chao Chen, MD, MS, 2 Ji-Chen Ho, M,3 Graduate Institute of Occupational Safety and Health, Kaohsiung Medical University; Department of Dermatology1 and Psychiatry2, E-Da Hospital / I-Shou University; Kaohsiung, Taiwan3 Department of Dermatology, Chang Gung Memorial Hospital-Kaohsiung Figure 1 The distribution and frequencies of malignant tumors in RTRs